
Translate this page into:
Cardiovascular Responses to Commonly Used Tests In and Outside of the Laboratory Settings
Address for correspondence Mohan B. Dikshit, MBBS, MD, FAMS, 48 Shivaji Housing Society, Senapati Bapat Road, Pune 411016, Maharashtra, India (e-mail: justmohan@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Several tests are available for assessing cardiovascular response to various interventions which may be given in the laboratory, or outside of it in the field. The tests are meant to excite or deactivate cardiovascular and other sensory receptors which signal the central mechanisms. They have been found useful in generating data to study cardiovascular effects on subjects exposed to specialized physical training (e.g., athletes), in the evaluation of people engaged in special occupations such as pilots, astronauts, and other military personnel, and in training undergraduate and postgraduate students. If the response does not fit into the physiological norm, it may reflect a temporary aberration, or a more serious defect in the cardiovascular control mechanism because of disease. Interpretation of data generated may vary between various operators/observers. Here, an attempt has been made to bring out responses of the cardiovascular system to the commonly used tests, and their applicability in clinical situations.
Keywords
cardiovascular system responses
central blood volume
cold pressor test
lower body negative pressure
exercise response

Introduction
The response of the cardiovascular system (CVS) to changing situations in body physiology is an integral part of the maintenance of the milieu interior. As to whether such a response is adequate or not may be studied in a physiology, or a clinical laboratory, or to that matter in field conditions, using a variety of tests or interventions (►Table 1). We have used such tests productively to study effects of various interventions on the CVS. For example, during sinus arrhythmia1,2 during exercise of varying intensities3,4,5; by displacing the central blood volume (CBV) to the periphery during quiet standing,1 as also by using head-up tilt (HUT),6,7 or the application of lower body negative (suction) pressure (LBNP/LBSP)8; and during an increase in the CBV applying 5-degree head-down tilt.9 We have also examined the effects of certain medications on the CVS response to stress applied by LBNP.10,11 Similarly, the effects of hand immersion in cold water1,12 with and without β blockade were investigated. With a series of experiments, we proposed that exposure of subjects on β-blocker (propranolol) to moderately severe heat stress as met with during tank operations by the Army during the summer while attenuating heat-induced cardiovascular strain, was unlikely to affect the individuals' heat tolerance.13 In another interesting experiment we attempted to decipher whether handedness influenced cardiovascular responses to a variety of autonomic stressors such as quiet standing, cold pressor test (CPT), hand grip dynamometry, and Valsalva maneuver1 but failed to draw concrete conclusions. We have thus been able to show that recording of the CVS response to various interventions may be gainfully employed for various physiological investigations and research as well as evaluation of individuals in specialized occupations. Needless to say, some of the tests are also used in clinical assessment of patients with heart disease, most importantly ischemic heart disease. This review, however, mainly concerns clinicophysiological aspects of the CVS test responses and their possible mechanisms and applications.
| 1. Tests in a resting subject: Deep breathing (for sinus arrhythmia) and heart rate variability (HRV) |
| 2. Exercise tests for cardiovascular system (CVS) intervention: (a) in the field: i. step test; ii. squat test; iii. hand grip dynamometry (isometric exercise). (b) Laboratory-dependent exercise tests; i. bicycle ergometry; ii. treadmill test |
| 3. Valsalva maneuver |
| 4. Depletion of central blood volume during (a) quiet standing; (b) head-up tilt; (c) lower body negative pressure (LBNP) |
| 5. Cold pressor test; mental arithmetic as influenced by higher centers |
Physiological Circuitry Involved in CVS Responses to Commonly Used Tests
A simplified concept of what transpires when common interventions use to stress the CVS and evoke a response is depicted in ►Fig. 1.
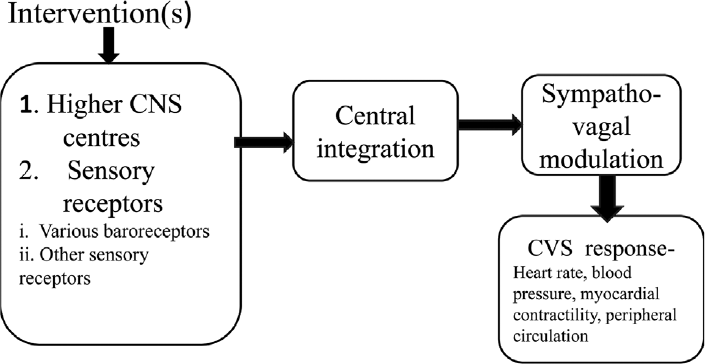
- Algorithm for cardiovascular system (CVS) responses to intervention(s) as a part of tests given.
The physiological inputs generated during the various tests will finally impinge upon the cardiovascular centers in the brain which in turn signal an optimal sympatho-vagal output to the CVS to obtain the desired result. The vagal or the sympathetic influence on the CVS at any particular time is governed by several central neurons located in the cerebral and limbic cortices, and the hypothalamus. These neurons are influenced by various sensory receptors in the periphery, namely, the cardiopulmonary and arterial baroreceptors, group III/IV afferent fibers in the skeletal muscles, chemoreceptors, and thermoreceptors. Such receptors are located in skeletal muscles, atria/ventricles, blood vessels, airway skeletal muscles, and the skin.14 The interactions thus generated determine the vagal and sympathetic outflows to the heart and the vasculature as required during a given test.
Various Tests as Outlined in ►Table 1 are Discussed Below
Tests in a Resting Subject
Sinus arrhythmia (SA) test, also known as respiratory SA (RSA), is a normal physiological phenomenon made prominent by deep relaxed breathing. It is best utilized as a test of autonomic control of the heart, its great advantage being its utility in patients who are unable to perform tests which induce a great deal of strain on the CVS. RSA is readily observed in children and young subjects where typically the heart rate (HR) increases during inspiration and reduces during expiration.1,15 It is accentuated by physical training16 and seen prominently in practitioners of yoga. Eckberg has attributed the phenomenon to an opening and closing of the respiratory gate which is brought about by the involvement of slowly adapting stretch receptors in the lungs, and the carotid baroreceptors.17 It reduces with advancing age, and in pathological conditions such as ischemic heart disease, hypertension, and diabetes mellitus.18 In the same context, it may be helpful in understanding the pathophysiology of coronavirus disease (COVID)-induced effects on the autonomic nervous system control of the heart in patients.
The test may be performed with a minimum of equipment by recording a long lead II on an electrocardiogram (ECG) machine while the subject breaths deeply at a rate of 6breaths per minute. Better still is a simultaneous recording of respiration and the ECG on a polygraph, best run at 10 mm/s so that long strips of recording may be viewed easily. The highest RR intervals of 5 to 6 beats (RR expiration) and those with lowest RR interval (RR inspiration) are obtained and expressed as the E/I ratio which, if it is 1.2 or more, confirms the presence of desirable SA. Similarly, the difference between the fastest HR (shortest RR interval) and the slowest rate (longest RR interval) should be 15 beats or more. In a group of healthy young medical students, we found the average E/I ratio to be 1.42, and the HRmax-HRmin to be approximately 17 beats.1
HR variability (HRV): A more accurate representation of SA is the measurement of frequency domains of the interbeat intervals derived from a fast Fourier transformation analysis. Three types of frequencies are measured as area under the curve (power spectral density)—very low frequency (VLF) band (< 0.04 Hz), low frequency band (0.04–0.15 Hz), and the high frequency (HF) band (0.15–0.4 Hz).19 The LF component indicates sympathetic activity while the parasympathetic influence is represented by the HF component. The VLF component has debatable physiological origins. A leaning toward HF is a sign of good vagal tone and heart health and is reflected as a prominent SA. A time domain analysis (standard deviation of NN intervals) which measures the standard deviation of interbeat intervals (N-N) can give an overall HRV status. However, this requires continuous recording of ECG with appropriate hardware which could extend up to 24 hours. ECG recording for up to 5 minutes at a time is also used. There are many technical requirements which need to be addressed if the HRV method is to be used successfully. Despite the limitations, HRV has been used to evaluate sympatho-vagal interactions in the heart under various interventions in normal subjects, as also in patients of myocardial infarction, those with transplanted hearts, and diabetic neuopathy.19
Exercise Tests as Commonly Used Cardiovascular Intervention
Prior to proceeding further, some commonly used terms as regards HR and blood pressure (BP) are deliberated upon below as these terms are often incorrectly attributed and described.
Resting HR and resting BP: These measurements are taken ideally when the person has been at complete rest for at least 10 minutes. The resting state is said to have been achieved when the R-R intervals between 5 and 6 consecutive beats, best measured at the end of a quiet expiration, are almost the same. This is particularly important when the test is being administered during a physiological intervention. Resting BP is recorded after complete rest, ideally in a semirecumbent or sitting position. Three consecutive readings, at 1-minute intervals, should be almost similar. The term Baseline or Control may be used in lieu of Resting especially during the conduct of physiological experiments when the change brought about by the intervention is being considered.
Peak HR and peak BP: These terms are particularly used during incremental exercise. The exercise is stepped up every 3 minutes. The HR (and BP) reached during the last minute of each step is the peak HR (and peak BP) for that level of exercise. The peak values of HR and BP represent the “steady state” reached during a particular level of exercise. In the clinical context, particularly while stress testing a patient suspected of suffering from ischemic heart disease, a peak or target HR to be achieved during the test may be set at 80% of the maximum HR for that person as decided by the age.
Maximum HR (HRmax): The HR during incremental exercise keeps on increasing until the individual is exhausted because of reaching maximum possible exertion that is linked to maximal oxygen consumption. At this stage, the HR does not increase further, and the individual is said to have achieved the HRmax. However, getting a subject to achieve HRmax is a rigorous process. This may be circumvented by a universally used regression equation generated by Fox et al20: HRmax = 220-age (years). Though simple to use, this equation may have overestimated the value in athletes, and underestimated it in the elderly. Some of these subjects were smokers while some were taking medication for cardiovascular disorders (Tanaka et al).21 These authors advocated that the parameter may be better estimated by the equation HRmax = (208–0.7 × age) usable in either sex. Smokers and/or those with CVS disease were excluded while deriving this equation. In a separate study, Gulati et al22 developed an equation for women in which HRpeak, as they called HRmax, is (206–0.88 × age). But when the various developed equations were compared, it was opined by Roy and McCrory23 that the one by Tanaka et al (HRmax = 208–0.7 × age) was best suited for use in both the sexes. However, the most popular equation in use remains 220-age. HRmax declines with age. It is possible that this decline is because of a decline in the intrinsic HR which may be obtained by a complete autonomic blockade and is independent of physical activity.21 The usual rate of decline is approximately 0.6 to 0.8 beats/min/year.
Rate pressure product (RPP) or double product (DP): This is obtained by multiplying systolic BP (SBP) by HR at rest and at various exercise workloads. It is usually expressed as [{SBP × HR}/100] to keep the number obtained at manageable levels; some divide the product by1,000. RPP is closely related to myocardial oxygen consumption (VO2).24 Values as reported by Sembulingam et al25 in young healthy males and females were around 120 mm Hg.beats/min at rest, and up to 220 mm Hg.beats/min during strenuous exercise. They considered this to be the normal range. When we calculated this parameter at rest from data in our various studies, we found an average of approximately 74 mm Hg.beats/min.1,4,6,7,9,10,11,12 In a cohort of 12 healthy young fighter pilots (mean age 35.7 years), the RPP calculated from available data was 359 mm Hg.beats/min at a maximal workload of 175 watts (1,067 kilopondals/min [kpm]) reached in an incremental manner on an electrically braked Monark bicycle ergometer from a resting average value of 82.6 mm Hg.beats/min.4 From this it is obvious that what may be designated as normal is vastly different. When interpreting exercise data, RPP may be expressed as DP factor (peak DP attained/resting DP) and DP reserve (peak DP-resting DP). If we derive the DP factor and the reserve in our study4 and that reported by Sembulingam et al,25 it is seen that the two derived parameters from our data are much higher (DP factor of 4.3 and DP reserve of 266 as against their DP factor of 1.83 and reserve of 100). It is possible that our subjects achieved maximal level of exercise while those in the other study performed at a much lower level of intensity. In patients with ischemic heart disease, Gobel et al26 suggested that abnormal increase in the DP may indicate poor myocardial health. Well-controlled exercise training in such patients helps by reducing the RPP at the same level of exercise suggesting clinical improvement. Complementing the findings of Gobel et al, Verma et al27 reviewed 7,141 congestive heart failure patients drawn from multiple centers around the world. They concluded that mortality was higher in patients who at the end of 30 days showed a greater increase in their resting RPP. Drawing concrete conclusions from this study as to the role of RPP as an indicator of myocardial VO2 becomes confusing as it is not clear whether increase in RPP is good or bad. Suffice to say that during physiological interventions in normal healthy subjects, an increase in RPP indicates good myocardial function.
Physiology of cardiovascular changes during exercise: The aim of the response of the CVS to exercise is to make available nutrients and oxygen to the exercising muscles by providing optimal perfusion. A simplified algorithm is outlined in ►Fig. 2.
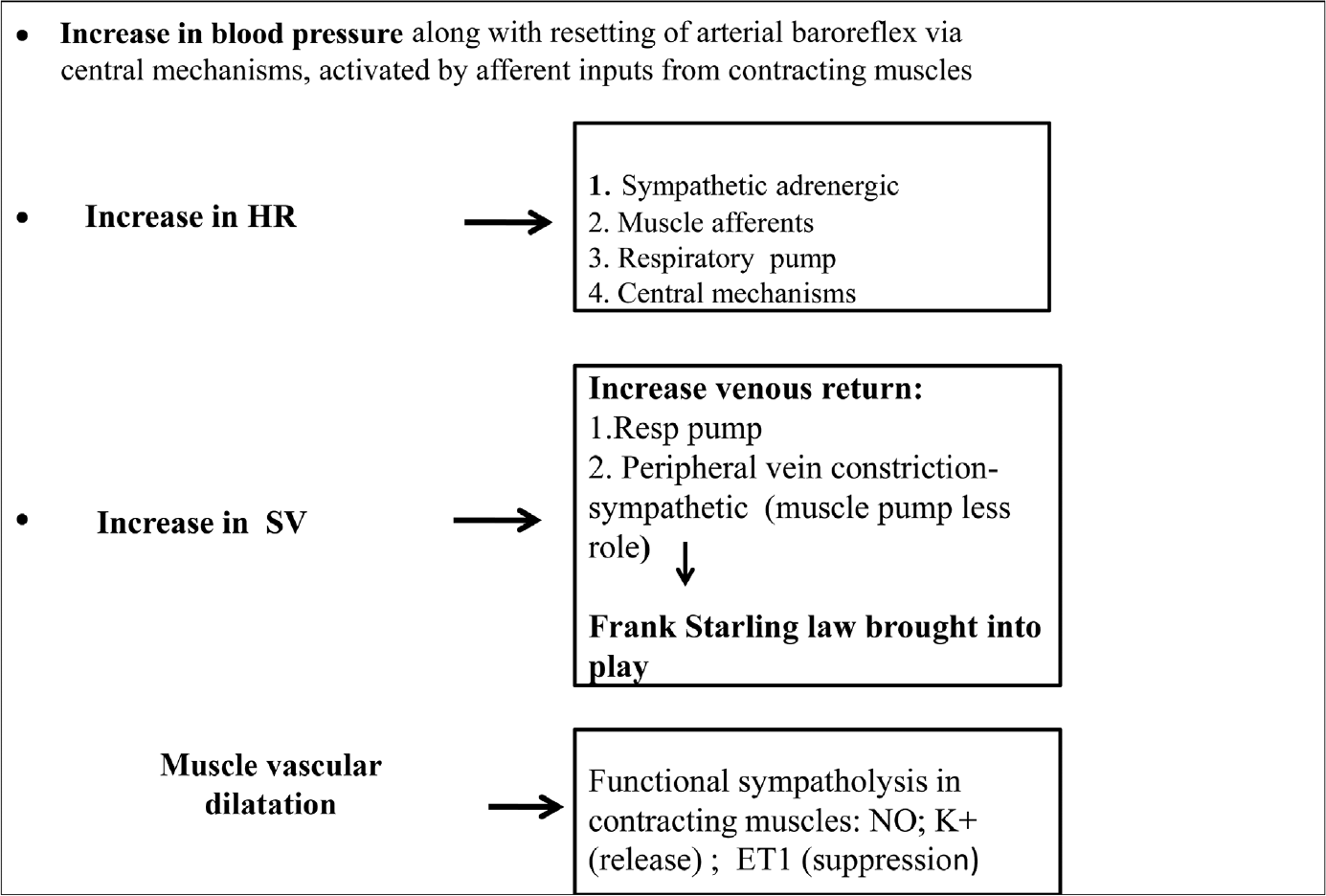
- Mechanisms involved in increasing perfusion of working muscles. The figure has been developed based on references 28–32.
To perfuse the contracting muscles, the blood flow to the contracting muscles increases manifold. This happens because of an increase in BP (predominantly the SBP to generate a propulsive force), an increase in HR, and a dilatation of muscle blood vessels to accommodate the extra flow. An increase in blood flow to the skin as a measure for attenuating an increase in body temperature must also occur though not discussed in this feature. While this is happening, the remaining organs must continue to get their fair share of the normal blood supply. Multiple mechanisms are in play to achieve the above.
The physiological axiom that an increase in BP must be followed by a decrease in HR and arteriolar vasodilation (Marey's law which describes the arterial baroreflex) is obviously undesirable during exercise. It is now known that this reflex is in fact “reset” to higher levels during exercise so that the desired BP rise continues to occur while at the same time retaining the protective ability of the system. This is brought about by two mechanisms: The feed-forward central command and the exercise pressor reflex.28,29,30
The feed-forward central command is the culmination of interaction between the higher brain centers (the motor cortex) and the medullary cardiovascular centers. This results in baroreflex resetting so that the HR continues to increase despite the concurrent BP increase. The exercise pressor response consists of the muscle mechanoreflex generated by group III/IV muscle afferents and the metaboreflex initiated by metaboreceptors in contracting muscles.29,30,31,32 The locally released metabolites such as adenosine, prostaglandin metabolites, and nitric oxide have been associated with a functional sympatholysis in the muscles which help in local vasodilatation.30 The afferent inputs from the metabo- and mechanoreceptors of the contracting muscles (the exercise pressor response) help the central feed-forward command to decide the degree of vagal withdrawal and the increase in the sympathetic drive. The desired increases in HR, stroke volume, and BP are thus achieved to ensure adequate cardiac output to working muscles.
Exercise response of a transplanted heart: This aspect is considered relevant here as patients who have undergone heart transplants may require a functional assessment. The exercise performance of a person with a transplanted heart is definitely compromised as compared with that of a normal person, particularly so during 6 months to 1 year after the transplant. Such a heart is devoid of any autonomic control. The resting HR is therefore intrinsic (at ∼100 beats/min), higher than that of a normal person.33 The rate of increase in HR during exercise is slow, and the peak HR achieved is limited. The power of contraction is also limited. As a result, the peak BP achieved during exercise is lower than expected. Whatever inotropic and chronotropic effects occur are dependent entirely upon the circulating catecholamines which are released as a part of the overall sympathetic activation.34,35 It was initially believed that the transplanted heart remains without reinnervation. However, more recently it has been indicated that reinnervation (both sympathetic and parasympathetic) does occur at last in some transplanted hearts over a period of time.33,36 This is usually evident by the end of a year as far as the sympathetic goes, while the parasympathetic may take 2 to 3 years. Parasympathetic reinnervation of the SA node is evidenced by the appearance of HRV while the fact that both the earlier onset of HR increase and the higher peak HR achieved at end exercise, as well a better stroke output suggests sympathetic reinnervation of the SA node as well as the left ventricle. Reinnervation has also been demonstrated using positron emission tomography.33 It may be noted that reinnervation is not the rule in all transplanted hearts.36
Cardiovascular response of the elderly to exercise: Life expectancy of Indians has gone up from approximately 40 years in the 1960s to approximately 70 years in 2020. With improving health care, this is likely to increase further. It is unfortunate that data pertaining to exercise response of relatively healthy elderly Indians is almost nonexistent, neither is any quotable information in Indian patients with heart disease and their exercise response available.37 Generation of such a database may be a useful activity to be taken up at physiology departments of various medical institutions in the country.
Studies elsewhere have indicated that in comparison with younger subjects, the CVS response during exercise is relatively compromised in the elderly (60 years and beyond). The main features of this change have been attributed to a limitation of the chronotropic response of the elderly.38,39 The HRmax in this group is known to reduce at approximately 0.7 beats/min/year.38 There is an increase in stroke volume because of increase in end-diastolic volume of the ventricles. However, the relative inability of body physiology in the elderly to augment HR limits the increase in cardiac output which occurs more easily in the young because of an increase in myocardial contractility.38,39 The less contractility in the elderly has been attributed by Roh et al38 to changes in the aging myocyte which includes disturbed handling of calcium, relatively dysfunctional mitochondria, and alterations in β adrenergic receptor sensitivity to circulating and locally released norepinephrine and its reduced reuptake. These are evidenced by a relatively unchanged end-systolic volume.39 The BP increase in the elderly is comparable to that of the younger subjects39 though this is intriguing as there is limitation of myocardial contractility as well as the HR response in the elderly. The redeeming feature is that exercise training improves the CVS responses of the HR and cardiac output, though these remain lower than what is seen in younger people.37,38 There is a suggestion that exercise training in the elderly may readjust sympatho-vagal balance of the heart as seen by a partial recovery of HRV in the postexercise phase. Both strength and endurance training are known to be helpful.40 An abnormal increase in BP during exercise is an indicator of endothelial dysfunction.41
Commonly used exercise tests: These tests, for the sake of convenience, may be divided into two categories: (1) tests which can be done at the clinic level/in the field with a minimum of equipment and (2) those done in a laboratory using sophisticated equipment like the bicycle ergometer or the tread mill.
Tests in the clinic/field: These simple to execute tests measure recovery HR after exercise to assess cardiorespiratory status. The YMCA 3-minute step test and the 45-second squat test fall into this category. The stress generated is at submaximal level (to attain a HR of ∼80% of the predicted HRmax for the individual). The tests may be used even in the elderly but with requisite safety precautions. The principle is that faster the recovery of the postexercise HR, better the sympatho-vagal balance indicative of a healthy heart and the CVS. Complications of using sophisticated machinery such as the treadmill (TM) or bicycle ergometer, recording of ECG, and measurements of BP are eliminated in these tests. Almost no costs are involved. Hand grip dynamometry may also be done at field level if the equipment is available.
The YMCA 3-minute step test: After at least 2 minutes of complete rest, the subject is made to step up and down on a 12-inch step at a rate of 24/minute.42 The timing may be adjusted after a demonstration by the observer, or by using a metronome if available. At the end of 3 minutes, the subject is made to sit down, and the HR is recorded for 1 minute thereafter. A pulse meter if available is most helpful. Absolute HR after 1 minute of exercise of approximately 90 beats/min in the young and up to 110 beats/min in those > 65 years indicates satisfactory fitness while lower values indicate better fitness. The response may also be deemed satisfactory when there is a reduction in 1 minute postexercise HR by approximately 25 to 30 beats/min. A drop by approximately 60 beats/min is considered as excellent fitness. Regression equations have been formulated to estimate oxygen consumption in Korean subjects using this test.42 The accuracy of the test in predicting fitness has been debated for various reasons. If the test is performed on individuals with varying leg lengths while using the standardized 12” step, the strain to which they would be exposed would be different because of the difference in biomechanics of stepping up and down. To avoid this and make the exercise comparable, the optimum hip angle at the time of stepping was estimated to be approximately 73 degrees. If this were not done, the height of the step would have to be different for different individuals.43 It was also argued that the fitness scores obtained could also vary depending upon the timing and duration of measurement of the recovery HR. Keeping these issues in mind, Santo and Golding44 attempted to redefine fitness scoring for the step test by measuring HRs in the 20 seconds at the end of exercise instead of the originally prescribed 1 minute post-recovery HR and using a variable height bench in which the step height was determined by the formula step Ht (height) = 0.192 × Ht in cm for males, and 0.189 × Ht in cm for females. In actual practice, however, in the field or in the clinic, these specifications may be difficult to adhere to. Nevertheless, the YMCA 3-minute step test still remains a very useful tool for measuring cardiovascular response to submaximal exercise in the standard format.
45-second squat test: This test was originally developed by Ruffier for testing CVS fitness in French and other European subjects. It was later validated by Guo et al45 in 40 U.S. subjects between the ages of 18 and 64 years. During the test, subjects are made to do 30 squats in 45 seconds. HR is recorded before test (P1), at the end of 45 seconds (P2), and 1 minute after the test (P3). The test score is calculated in the form of an index—the Ruffier's Index (RI) expressed as ((P1 + P2 + P3) – 200)/10, and modified further as the Ruffier–Dickenson Index (RDI) = ((P2–70) + 2(P3–P1))/10. One of the main criticisms of this work (also conceded to by the authors) is the relatively small number of subjects—18 males and 22 females. Also, this small group may or may not be representative of the overall American population. The range of the RI given was 2.5 to 17.1 (average 8.9) for males and 4 to 23.4 (average 10) for females, while the RDI scores were 5.5 to 18.4 (average 10.8) for males and 5.4 to 22.2 (average 10.8) for females. One may then assume that those who have scores toward the lower limits have a very good fitness while those who are in the upper ranges have a lower fitness grade. It may be deduced that the VO2max is inversely related to these scores. However, the authors did not find a direct relationship between the two indices and the maximum oxygen consumption. They derived complex equations using age, height, sex, and P1, P2, and P3 values to derive the regressions for VO2max which correlated quite well with the direct VO2max measurements using a modified Balk protocol on the TM. These gave a specificity and sensitivity of around 80 and 60%, respectively. Considering the available information, one may opine that the squat test is easier to use in the field given that one can actually calculate a degree of fitness by obtaining the RI and RDI, and that there is no requirement of even a stepping bench with its vagaries of height. It would be useful to generate such data in both healthy Indian males and females, and later apply it to patients with heart disease, mainly ischemic heart disease.
Again, there is a dearth of information on Indian subjects of various age groups as regards these simple tests. With the current interest that is being generated in our country about sports, collection of cardiovascular response data using such tests may be of relevance.
Laboratory-Dependent Exercise Tests
Cycle ergometry (CE) and the TM: Sophisticated cardiovascular tests where the final aim is to measure VO2max are given by using the electrically braked bicycle ergometer or the TM. The advantage of using these equipment is that the stress may be given in a graded (step-wise) manner (submaximal exercise) which may then be progressed to the maximal exercise capacity of the individual. Throughout the procedure, various cardiovascular parameters (ECG, HR, BP, etc.), respiratory parameters such as respiratory rate, tidal volume, and metabolic parameters (VO2 and VCO2, metabolic equivalents) may be recorded online given the availability of suitable equipment. We have observed that the BP recording when made manually is easier done on the bicycle ergometer. On the TM, more often than not, it is difficult to hear the diastolic signal of the sphygmomanometer because of the thumping produced while the individual walks/runs on the TM.
As a rule, we are used to presume that, when we walk, the earth below is static while we are moving in a given direction on it. For the ab initio user of the TM, the fact that now the ground below one's feet is moving and that one is required to keep pace with it to avoid stumbling is slightly disconcerting to begin with. In most instances though, the change is rapidly adjusted to. This change over can be further helped by starting the TM at a low speed while the walker keeps watching a picture/scenario hung up at eye level in front of him/her. Ideally, when a subject settles down to the rhythm of the TM, it is best to walk/run without holding the TM rails for support as this then simulates the natural process of the movement as far as possible. For a given degree of cardiovascular stress, the VO2max during TM testing may be higher by 6 to 25%46 while Patton et al47 found it to be approximately 16% higher in both young males and females. The latter's findings of comparable VO2max values, however, seem to suggest that TM may be a better method of assessing cardiovascular fitness in males. The correlation of VO2max with both TM and CE is better in males.48 The TM puts stress on moving joints of the lower limbs and hence is best avoided with people with osteoarthritis or joint injuries/disabilities of the lower limbs. It may lead to balancing problems, particularly in the elderly, at the start, during change of speed, and on stopping the machine, particularly so if this has to be done suddenly because of an emergency. These issues are avoided with a bicycle ergometer. The other advantage of the CE is its easy mobility from place to place, and cheaper cost of installation and maintenance. In suitable candidates, one or the other may be used to generate cardiovascular stress,49 though TM seems to be the method of choice.50 For physiological experimentation/evaluation in human subjects, we have been more familiar with the use of CE.4,5 We have generally used a pedaling speed of 60/min before applying the load (watts or kpm). The load may be applied electrically or mechanically. The former is the method of choice. Application of mechanical resistance to the flywheel rotations may reduce with time as the tensile strength of the band material may decline. The other minor issue with CE is the setting of pedaling rate. We have been using 60/min while 75/min may also be used. The pedaling rate needs to be attained prior to giving the load. There after the subject may need goading to maintain the set rate as the workload increases. A similar issue though of less magnitude may also be experienced on the TM where a subject may require encouragement to keep pace with the TM speed.
Hand grip dynamometry helps in eliciting a cardiovascular response to isometric exercise. The CVS effects are a result of activation of the muscle metaboreflex and the muscle mechanoreflex brought about by powerful isometric contractions of the forearm muscles, and a central command which may modify the CVS response to any given degree of muscle contraction via the cardiovascular centers.51 Physiologically then, this may be classified as an exercise stress test. To perform the test, the subject first generates a maximum force by squeezing the dynamometer (usually of a range 0–100 kg), and sustains it for approximately 4 to 5 seconds. The maximum value (kg) achieved is recorded. The subject is then asked to squeeze the dynamometer to a fixed percentage of the maximum achieved. For example, we have used 30% of the max force achieved maintained for 2 minutes1 while others have used 40% max force generated until the subject is unable to sustain the effort.51 In the elderly, the force which needs to be generated may be reduced to 20% of max achievable. The basic variables such as HR and BP are best recorded online. Muscle sympathetic nerve activity (MSNA) may also be monitored.51 Typically, the HR and BP increase rapidly to peak level at the end of the test (2 minutes), and return toward resting values on cessation of the exercise. The test may be used in evaluating response of the CVS in clinical conditions, in sports medicine and physiotherapy departments, or as intervention to study physiological phenomenon, as we have, to compare responses of difference in handedness,1 or for evaluation of effects of space flight.51
Tests which induce a CVS response when the CBV is depleted: The commonly used tests are: (1) quiet/passive standing; (2) HUT test; and (3) LBSP/LBNP. The principle used in these tests is to produce a gravity-induced displacement of the CBV into the lower limbs during standing and HUT, or use suction to pull it down into the lower limbs using LBNP,1,7,8 thereby inciting the system to respond by bringing in corrective reflexes in terms of increase in HR and BP, as also the contractility of the myocardium. Greater the volume displaced and longer the time for which this displacement persists, greater is the stress on the CVS. Using these methods, we have studied CVS responses of right-handed subjects versus left-handed ones1; evaluated cosmonaut candidates4; studied the effects of various medications which affect the CVS10,11; and clinically assessed apparently healthy individual with history of vasovagal syncope, or postural orthostatic tachycardia syndrome (POTS).7,52
Quiet/passive standing test: On standing, approximately 600 to 800 mL of blood from the thoracic cavity is shifted into the lower limbs because of gravity. The typical response to standing from a supine position is depicted in ►Fig. 3.

- Immediate response to standing from a supine position recorded online.52
Visualizing in slow motion, there is a sudden fall in SBP as the thoracic cavity is deprived of a fairly large part of the CBV. As this volume rapidly fills the blood vessels below the heart level, there is a distension of the vasculature below heart level which is seen as an initial decrease in the total peripheral resistance (TPR) (Fig. 3). The saving grace which tries to overcome this fall in the BP is the rapid vagal tone withdrawal which sets off an increase in HR. This is followed within a couple of seconds by an increase in TPR brought about by myogenic vasoconstriction. In the subsequent 8 to 10 seconds, deactivation of the carotid arterial baroreceptors brings about reflex sympathetic activation in support of the initial responses, stabilizing the overall perfusion by approximately 30 seconds. The TPR is now maintained by sympathetic vasoconstriction, while the venous return is aided by the thoracic pump. Despite these reparative steps the stroke volume and the cardiac output remain below prestanding levels, while a slow depreciation in the CBV continues.53,54,55 Stabilization is completed by approximately 30 seconds. It is best to record the CVS parameters on line as in ►Fig. 3 while supine, immediately on standing, and thereafter at 1-minute intervals for at least 5 minutes.1 The duration may be extended to 20 minutes. If specialized facilities are not available, a standard BP apparatus may be used. Care must be taken to inflate the BP apparatus cuff before the subject changes posture for obvious reasons. Another observer may then record the HR at the precordium using a stethoscope. This simple test is useful for initial data collection in the field or for early evaluation of a suspected case of vasovagal syncope/POTS before referral to an advanced laboratory for detailed investigations.
HUT test: This is by far the most extensively used test for the evaluation of orthostatic tolerance. A typical response of normal young Indian males is depicted in ►Fig. 4. The principle of applying the test is that the CVS is the same as that of standing: displacement of CBV of approximately 600 to 800 mL into the lower limbs. The advantage of HUT over standing is that the subject concerned does not have to make any effort, and recording is not disturbed while giving the HUT as it may happen in the standing test. Various degrees of HUT from 30 to 90 degrees have been used. The tilt may also be given in a graded manner to produce different amounts of sequestration of the CBV. Tilt angle of 70 degrees is by far the most commonly used as it produces fluid displacement similar to quiet standing. The hydrostatic effect of the blood column is determined by the tangent of the tilt angle which is 1 when fully upright (90 degrees) when the hydrostatic column exerts the maximum pressure at the level of the feet. At 70-degree tilt this tangent value is almost 1, and is thus most acceptable compromise between the ideal and the pragmatic.56 The rate at which the HUT is applied determines the rate of displacement of the blood into the periphery and hence the onset of the CVS reflex response. If given too rapidly, vestibular stimulation may distort the CVS response. Most laboratories now use an electrically operated tilt table which achieves the set angle in approximately 15 to 20 seconds. The duration of the HUT may vary from 5 to 20 minutes or more. Longer the duration (beyond 20 minutes) greater the possibility of a syncope even in normal subjects as CBV sequestration increases to well beyond the usual 600 to 800 mL despite the protective reflexes.
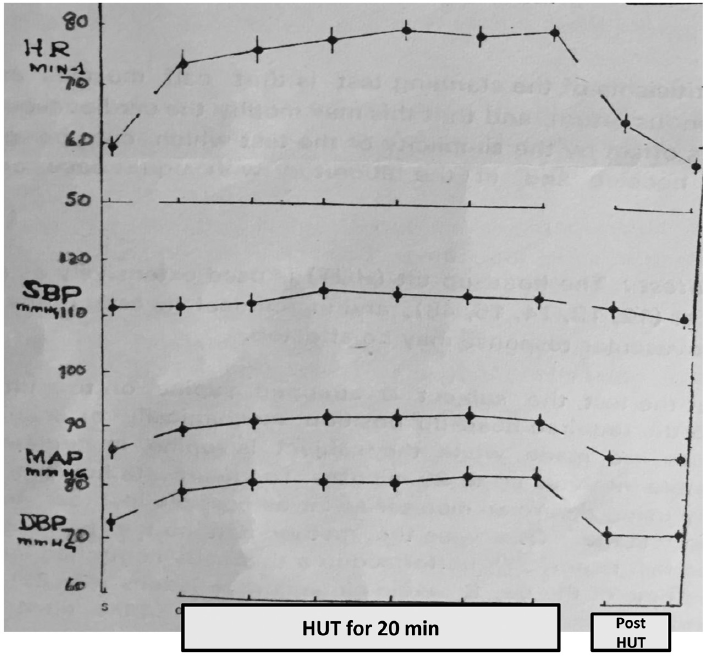
- Cardiovascular system (CVS) response of normal young males to 70-degree head-up tilt (HUT).56
LBSP/LBNP was introduced by Duane Gavelin (for space flight research), followed by Professor A.D.M. Greenfield in the early 1960s to study the effects of shifting of CBV without a change in the supine posture. Since then, it has been used extensively in cardiovascular research.
The suction may be applied by using a vacuum cleaner, placing the subject in the supine position in a rigid box with a rubber seal at the level of the iliac crest. The biggest advantage of using LBNP which may vary from –10 to –60 mm Hg is that the suction can be applied in a graded manner in a supine subject. Even though the possible vestibular stimulation during a rapid HUT is absent during LBNP, we have been able to demonstrate the appearance of mild, spontaneous but significant slow nystagmus during suction of around –50 mm Hg. This may happen because of a possible involvement of the nystagmus generator in the midbrain. Its possible influence on the CVS response to LBNP is unknown.57 At about –50 mm Hg, the central volume displacement is similar to that while standing or during HUT. The lower levels of suction pressure (below –20 mm Hg) have been used to deactivate low pressure cardiovascular receptors.10,56 However, the natural physiological stimulus which is the effect of gravity in bringing about fluid shift, is absent. It is perhaps this aspect which is responsible for the slight differences in response of normal healthy young men to LBNP and HUT. For example, in our series of HUT tests in 143 military men, the average increase in HR and diastolic BP (DBP) was 16 beats/min and 9 mm Hg, respectively, while the SBP fell by just 1 mm Hg.7 On the other hand, in another group of young military men exposed to –50 mm Hg LBNP the HR and DBP increased by 9 beats/min and 3 mm Hg while the SBP fell by 7 mm Hg.11 Keeping in view our findings that mild nystagmus is often seen during LBNP level of –50 mm Hg,57 one may speculate that this could also be a possible factor for the slight differences in response to LBNP as compared with that seen during HUT. A combination of HUT and LBNP applied simultaneously has been used to stress the CVS,58 but we have had no experience of this, nor do we advocate its use as we believe that nothing more may be gained by the procedure except to expose the subject to greater discomfort.52 Some subjects may feel a sense of being pulled downwards, especially at pressures of –50 mm Hg, and more so if the rate of application of suction is fast. For detailed information on LBSP, the reader may refer to an excellent review by Goswami et al.59
Valsalva maneuver: This test was initially introduced by Antonio Valsalva, an Italian Anatomist in the 17th century to study the Eustachian tube. It is now almost invariably used by ear, nose, and throat surgeons to do a quick assessment for Eustachian tube patency. Its more specific use is made in the study of the cardiovascular control mechanisms and of the adequacy of left ventricular function. The standard method of performing the maneuver (for assessing CVS status) has been described elsewhere.1 A respiratory trace may be recorded to ensure sustenance of the expiratory effort. Cardiovascular parameters (ideally online) are recorded during the breath hold and after releasing the breath. Alternatively, the subject may be asked to breath out into a mercury manometer so that the Hg column is raised to and maintained at 40 mm Hg for 30 seconds (or longer) (historically referred to as the “40 mm Hg test” in Air Force medical circles all over the world). The index that is calculated is the Valsalva ratio (maximum HR during the maneuver/minimum HR on termination). The expected value in a normal response is approximately 1.5 and more.60 In our series of 28 young healthy medical students (14 right-handed and 14 left-handed), the ratio obtained was1.49 ± 0.41for right-handed and 1.59 ± 0.43 for the left-handed (for both 1.52).1
After the first 5 to 7 seconds of starting the maneuver, an increase in HR and DBP with little or no change in SBP is caused by reflex sympathetic activation secondary to arterial baroreceptor deactivation. The reflex is triggered by a reduction in venous return produced by the raised intrathoracic pressure. This persists as long as the test continues. The rebound decrease in HR on release of the pressure indicates a sudden increase in vagal discharge because of the increase in stroke output and systolic pressure. The latter two effects are considered indicators of good left ventricular function and a healthy ratio is indicative of a sound carotid baroreceptor reflex pathway. It is suggested that Valsalva could be used along with orthostatic tolerance tests in the evaluation of vasovagal syncope episodes. A modification of the Valsalva, breathing out forcibly through a partially closed glottis with straining of abdominal muscles,61 is taught to fighter pilots to increase their tolerance to positive accelerations (+Gz).
Clinical use of Valsalva maneuver for assessing CVS function, particularly left ventricular function, has been in vogue but perhaps not as extensively used. Levin60 has suggested that the data generated using Valsalva test in patients of valvular heart disease is as useful for assessing cardiac function as that obtained with cardiac catheterization. In 220 patients he reported that greater the severity of dyspnea and the valvular lesion, lower the Valsalva ratio. During the second phase of the maneuver, when the venous return, and consequently left ventricular filling, have been reduced, systolic murmurs secondary to cardiomyopathy may be heard more prominently on auscultation. Further, during phase IV, auscultation may be able to differentiate between right heart and left heart murmurs as the right-sided ones appear early within the first two beats while the left-sided ones appear after a few more beats.62 Clinical examination using the maneuver is thus likely to be helpful in cardiac assessments of patients with murmurs when more sophisticated facilities such as echocardiography may not be available. Others have found the maneuver useful in studying patients with patent foramen ovale large enough to produce right to left shunts of various degrees.63 The test is best done in combination with specialized investigations such as transesophageal electrocardiography, transthoracic echocardiography during microbubble insertion, and transcranial Doppler. Yet, others have recommended the use of the maneuver for noninvasive, bed side assessment of patients of congestive heart failure64 because the CVS response to Valsalva maneuver reveals efficiency of left ventricular function.
Tests Influenced by Higher Centers
The CPT was introduced by Hines and Brown in 1932 seemingly to investigate “The reactivity of the BP: data concerning 571 normal and hypertensive subjects.” It was first reported in the American Heart Journal of 1936 (Vol. 11: pp. 1–9). The test is given by immersing the hand up to the wrist in ice cold water at approximately 4 to 5°C for 2 to 4 minutes as we have been doing.1,4,12 Immersion of either one or both feet up to the ankle has also been used. It is felt that immersing foot/feet leaves the subject's hands free to carry out any given tasks, or makes him/her feel more at ease, and may help in reducing cortical bias, and is most feasible when both feet are used.65 Immersion of both the feet may invoke greater stress and hence more pronounced sympathetic activation.66 Various CVS variables (HR, BP, RPP, cardiac output, coronary artery diameter,1,4,12,67 and MSNA) may be recorded.51,68 Depending upon available laboratory facilities, recordings of the physiological variables are best done either online, or at half-minute intervals for 2 minutes as we have been doing,1,4,12 with postimmersion follow-up for approximately 2 minutes.
The CPT invokes a powerful sympathetic excitation brought about by stimulation of skin cold nociceptors in the hand (or the foot) stimulated by the ice-cold water. The painful afferent signals are carried by C fibers to the central nuclei which are known to control sympathetic outflow. There is probably a wide-ranging interaction between the various higher centers including the sensory cortex, the limbic system, and finally the CVS centers51,68 which are finally translated into CVS and MSNA responses. The CVS response to the CPT varies markedly among subjects/patients. Various factors such as genetic, physical fitness, ethnicity, age, sex, pain threshold, obesity, and inter- and intraindividual variation69,70,71,72,73,74 are known to influence it.
The HR response to CPT has been known to vary from no change to a rapid increase in the first 30 seconds followed by a gradual return toward base line by end of immersion, or a sustained increase throughout the cold immersion.1,4,75,76 It has been reported that the MSNA increase comes into play after approximately 30 seconds of hand immersion in cold water.74,77 What then is the explanation for initial rapid increase in HR? It could be because of a sudden spill of catecholamines into the blood67 or a vagal withdrawal as proposed by Mourot et al.76 It has been suggested that baroreceptor function is reset during the CPT.74 This may then explain as to why the HR after an initial increase tends to come down as the CPT progresses. Perhaps in those in whom the HR continues to be high, the baroreceptor resetting is delayed. The BP shows a consistent increase during the test. The initial increase in the first 30 seconds has been attributed to the increased HR alone as the stroke output does not change.75 However, there are other reports which have highlighted increased cardiac contractility contributing to the increase in cardiac output, but in athletes, and not in untrained normal young subjects.72 The MSNA, which comes in to play after approximately 30 seconds of cold immersion,74,77 is probably the cause of the raised BP after approximately 30 seconds during the immersion. In our young healthy male medical students1 and fit military men,4 both the SBP and DBP showed a consistent increase during the test while the HR followed the more conventional norm of a rapid increase followed by a gradual decrease to near pretest levels. Against this, in our young Caucasian medical students (4 males and 3 females) there was a negligible HR increase, and while the BP (SBP and DBP) increased in the early stages, it returned toward pretest even during the test.12 The BP changes occurred in these subjects even after having been given 120 mg propranolol 2 hours prior to the test. That the drug had acted as expected was evident because of the much lower pretest HR in the propranolol regimen (mean HR 58 vs. 74/min without the drug). Perhaps ethnicity may be the explanation.
The main feature of the CPT which is translated into CVS response is the increase in MSNA.51,77 This increase is independent of the baroreceptor reflex as suggested by Cui et al.74 Fagius et al78 reported enhanced MSNA with greater pain sensation. From this it may be concluded that depending upon the perception of pain, the degree of MSNA recorded is bound to vary among individuals, and this in turn would explain the wide variation of CVS response to the test.
CPT has been used as an intervention to study various phenomenon such as effects of space flight,51 responses to various situations such as high-altitude acclimatization, cold adaptation, and clinically in provocation of coronary artery disease as brought out by Dikshit and Patrick.79 Monahan et al67 have cautioned that the coronary vasodilatation which normally occurs during CPT in young people probably because of release of an endothelium-derived relaxing factor and excitation of β2 adrenergic receptors by circulating catecholamines, may be poor or absent in the elderly. And hence use of this test in the elderly and before applying in those with a history of ischemic heart disease may have serious repercussions. Pain perception and pain sensitivity have been investigated using this stress test.80,81 In fact, McIntyre et al81 have suggested its use in deciphering suitability of clinical use of opioids. By far the most elaborate use of the CPT has been made to identify the so-called “hyperreactors” to the test for potential hypertensives. In fact, the test was originally designed by Hines and Brown in 1932 to test this hypothesis. The results have however been quite confounding. Some have strongly favored the hypothesis that hyperreactors to the CPT are in fact potential hypertensives82,83 while others have opined that no correlation could be established.84 Jaju70 in her study of Omani Arab families with history of high BP found the test inconclusive in establishing that hyperreactors may in fact go on to develop hypertension. Hubli et al85 have used it to study the reflex vascular reactions in patients with spinal cord section. Considering the various views, the observers using the CPT must be wary of interpreting the results of this test. Undoubtedly though, a “normal” response to the test is highly indicative of a robust efferent arm of the sympathetic neural reflex. Its use in patients of prevalent or suspected cardiovascular disease has to be carefully deliberated upon because of the intensity of sympathetic response it evokes.
Mental arithmetic is a simple method of stressing the CVS. The subject is asked to rapidly subtract, usually an odd number, from a starting point, say 1,000. The subtraction number may be changed after every 15 to 20 seconds during the test which lasts for approximately 3 to 5 minutes. Cardiovascular variables are recorded. There is a consistent increase in HR and BP as the test progresses. Males show a greater rise in BP compared with females while the MSNA response is quite variable and debatable. As to the reason as to why the latter may or may not be activated is not clear.86 The significant increase in blood catecholamines during mental arithmetic has been attributed to a powerful activation of the sympatho-adreno-medullary system.87 One drawback to these findings could be that the study was performed in hypertensives without normal controls. Studies have shown that the left-sided parietal and temporal cortices are mainly involved in the CVS response to mental arithmetic.88 The test has been found to be useful in diagnosing patients with white coat hypertension89 but there is no reason to presume that it could be better than other CVS stress tests such as the CPT. Its main advantage is that no equipment is required to give the test, and that the CVS response is fairly reproducible.90 It has been found useful for investigating patients of angina91 as it is physically less stressful to the patient, and hence in this context, could be a useful test for investigating cardiovascular reflex status as a follow-up of patients of COVID 2 while investigating pathophysiology of this viral disorder.
Conclusion
Several tests may be given to evoke the cardiovascular responses in the field, in the clinic, and/or in sophisticated laboratories. In the Indian context, little information is available about CVS responses to various tests in the elderly population. Given that the life span of Indians is on the rise, this lacuna could be addressed by various physiology and geriatric departments in the country to have a better insight into stress responses of CVS of senior citizens in good health, and in those with cardiovascular disease. Similarly, more and more young women are venturing in to high-intensity sports and in military professions. Here too we have a dearth of information on cardiovascular stress responses. Some of the tests may be useful in assessing patients with cardiovascular diseases. Here too Indian medical literature is deficient. Of particular significance may be the investigation of the autonomic nervous system involvement in patients with long severe acute respiratory syndrome COVID-19 infection.
Acknowledgments
Prof. Chandrasekhar Apte, HoD Physiology, College of Medicine and Health Sciences, National University of Science and Technology, Suhar, Oman made helpful comments. Mr. Mohit Dikshit is thanked for editing the final manuscript.
Conflict of Interest
None declared.
References
- Heart rate and blood pressure responses of left-handers and right-handers to autonomic stressors. Indian J Physiol Pharmacol. 2004;48(01):31-40.
- [Google Scholar]
- The mirage that is sinus arrhythmia. Abs. Proceedings of the International Conference on Cardio-pulmonary Regulation in Health and Disease: Molecular and Systemic Integration. 22–24; VP Chest Institute University of Delhi 2007 February:5.
- [Google Scholar]
- Medical evaluation of cosmonauts: physiological stress testing. Aviat Med. 1984;28(02):107-115.
- [Google Scholar]
- Cardiovascular response of patients of mild asthma to maximal exercise. J Assoc Physicians India. 1988;36:45.
- [Google Scholar]
- Comparative cardiovascular response to 70° head up tilt in pilots and non-pilots. Aviat Med. 1983;27:36-42.
- [Google Scholar]
- Orthostatic tolerance of normal Indians and those with suspected abnormal cardiovascular reflex status. Aviat Space Environ Med. 1986;57(02):168-173.
- [Google Scholar]
- Lower-body suction and cardiovascular reflexes: physiological and applied considerations. Indian J Physiol Pharmacol. 1990;34(01):3-12.
- [Google Scholar]
- Vital capacity and airflow measured from partial flow-volume curves during 5 ° head-down tilt. Aviat Space Environ Med. 1987;58(04):343-346.
- [Google Scholar]
- Human orthostatic reflexes after taking temazepam at night. Br J Clin Pharmacol. 1987;24(06):799-807.
- [Google Scholar]
- Calcium channel blockers and the CVS reflex responses during lower body suction. Indian J Physiol Pharmacol. 1991;35(04):232-236.
- [Google Scholar]
- Flow-volume curves during hand immersion in water at 5 ° C (the cold pressor test) Bull Eur Physiopathol Respir. 1986;22(03):269-272.
- [Google Scholar]
- Beta-adrenoreceptor blockade attenuates heat-induced tachycardia, but not the tolerance to the stress. Indian J Physiol Pharmacol. 1992;36(03):149-154.
- [Google Scholar]
- Neural control of the circulation. Adv Physiol Educ. 2011;35(01):28-32.
- [CrossRef] [PubMed] [Google Scholar]
- Respiratory sinus arrhythmia: why does the heartbeat synchronize with respiratory rhythm? Chest. 2004;125(02):683-690.
- [CrossRef] [PubMed] [Google Scholar]
- Respiratory sinus arrhythmia alteration following training in endurance athletes. Eur J Appl Physiol Occup Physiol. 1992;64(05):434-436.
- [CrossRef] [PubMed] [Google Scholar]
- Respiratory sinus arrhythmia and diseases of aging: obesity, diabetes mellitus, and hypertension. Biol Psychol. 2007;74(02):212-223.
- [CrossRef] [PubMed] [Google Scholar]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Circulation. 1996;93(05):1043-1065.
- [Google Scholar]
- Physical activity and the prevention of coronary heart disease. Ann Clin Res. 1971;3(06):404-432.
- [Google Scholar]
- Age-predicted maximal heart rate revisited. J Am Coll Cardiol. 2001;37(01):153-156.
- [CrossRef] [PubMed] [Google Scholar]
- Heart rate response to exercise stress testing in asymptomatic women: the St. James Women Take Heart Project. Circulation. 2010;122(02):130-137.
- [CrossRef] [PubMed] [Google Scholar]
- Validation of maximal heart rate prediction equations based on sex and physical activity status. Int J Exerc Sci. 2015;8(04):318-330.
- [Google Scholar]
- Rate pressure product responses during an acute session of isometric resistance training: a randomized trial. J Hypertens Cardiol. 2017;2:1-11.
- [CrossRef] [Google Scholar]
- Rate pressure product as a determinant of physical fitness in normal young adults. J Dent Med Sci. 2015;14:8-12.
- [Google Scholar]
- The rate-pressure product as an index of myocardial oxygen consumption during exercise in patients with angina pectoris. Circulation. 1978;57(03):549-556.
- [CrossRef] [PubMed] [Google Scholar]
- Rate pressure product and the components of heart rate and systolic blood pressure in hospitalized heart failure patients with preserved ejection fraction: insights from ASCEND-HF. Clin Cardiol. 2018;41(07):945-952.
- [CrossRef] [PubMed] [Google Scholar]
- Arterial baroreflex resetting during exercise: a current perspective. Exp Physiol. 2006;91(01):37-49.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiac autonomic responses during exercise and post-exercise recovery using heart rate variability and systolic time intervals-a review. Front Physiol. 2017;8:301.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular reflex activity and their interaction during exercise. Biomed Res Int. 2015;2015:394183.
- [CrossRef] [PubMed] [Google Scholar]
- Muscle metaboreflex control of the circulation during exercise. Acta Physiol (Oxf). 2010;199(04):367-383.
- [CrossRef] [PubMed] [Google Scholar]
- Neural regulation of cardiovascular response to exercise: role of central command and peripheral afferents. Bio Med Res Intern. 2014;2014:478965.
- [CrossRef] [PubMed] [Google Scholar]
- Bergin JD. Competitive athletics after heart transplant. Amer Coll Cardiol. 2016;172:96-105.
- [Google Scholar]
- Responses of the cardiac transplant patient to exercise and training. Exerc Sport Sci Rev. 1992;20:297-320.
- [CrossRef] [PubMed] [Google Scholar]
- Exercise after heart transplantation: an overview. World J Transplant. 2013;3(04):78-90.
- [CrossRef] [PubMed] [Google Scholar]
- Early denervation and later reinnervation of the heart following cardiac transplantation: a review. J Am Heart Assoc. 2016;5(11):e004070.
- [CrossRef] [PubMed] [Google Scholar]
- Exercise in the management of coronary artery disease. Med J Armed Forces India. 2007;63(04):357-361.
- [CrossRef] [PubMed] [Google Scholar]
- The role of exercise in cardiac aging: from physiology to molecular mechanisms. Circ Res. 2016;118(02):279-295.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular responses to exercise: effects of aging and exercise training in healthy men. Circ Res. 2016;118(02):279-295.
- [Google Scholar]
- Effects of exercise on cardiovascular performance in the elderly. Front Physiol. 2014;5:51.
- [CrossRef] [PubMed] [Google Scholar]
- The determinants of blood pressure response to exercise. Cor Vasa. 2015;57(03):e163-e167.
- [CrossRef] [Google Scholar]
- The validity of the YMCA 3-minute step test for estimating maximal oxygen uptake in healthy Korean and Vietnamese adults. J Lifestyle Med. 2020;10(01):21-29.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of limb length on a stepping exercise. J Appl Physiol. 1978;44(03):346-349.
- [CrossRef] [PubMed] [Google Scholar]
- Predicting maximum oxygen uptake from a modified 3-minute step test. Res Q Exerc Sport. 2003;74(01):110-115.
- [CrossRef] [PubMed] [Google Scholar]
- A 3-minute test of cardiorespiratory fitness for use in primary care clinics. PLoS One. 2018;13(07):e0201598.
- [CrossRef] [PubMed] [Google Scholar]
- Exercise testing methodology. In: Exercise and the Heart. Chapter 2.5th ed. London: Elsevier; 2006:11-39.
- [CrossRef] [Google Scholar]
- Evaluation of a maximal predictive cycle ergometer test of aerobic power. Eur J Appl Physiol Occup Physiol. 1982;49(01):131-140.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of treadmill versus bicycle ergometer training on functional exercise capacity in normal individuals. Int J Cur Res Rev. 2014;6(10):61-65.
- [Google Scholar]
- Treadmill and cycle ergometer tests are interchangeable to monitor triathletes annual training. J Sports Sci Med. 2003;2(03):110-116.
- [Google Scholar]
- Energy expenditure with indoor exercise machines. JAMA. 1996;275(18):1424-1427.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular and sympathetic neural responses to handgrip and cold pressor stimuli in humans before, during and after spaceflight. J Physiol. 2002;544(02):653-664.
- [CrossRef] [PubMed] [Google Scholar]
- Current concepts of pathophysiology of vasovagal syncope and its evaluation and management: a review. Ann Natl Acad Med Sci. 2018;54(03):120-146.
- [CrossRef] [Google Scholar]
- From supine to standing: in vivo segregation of myogenic and baroreceptor vasoconstriction in humans. Physiol Rep. 2016;4(24):e13053.
- [CrossRef] [PubMed] [Google Scholar]
- A definition of normovolaemia and consequences for cardiovascular control during orthostatic and environmental stress. Eur J Appl Physiol. 2010;109(02):141-157.
- [CrossRef] [PubMed] [Google Scholar]
- Blood pressure and blood flow variation during postural change from sitting to standing: model development and validation. J Appl Physiol (1985). 2005;99(04):1523-1537.
- [CrossRef] [PubMed] [Google Scholar]
- Postural stress tests for the clinico-physiological evaluation of cardiovascular reflexes. Indian J Physiol Pharmacol. 1987;31(01):1-11.
- [Google Scholar]
- Combined head-up tilt and lower body suction: a test of orthostatic tolerance. Clin Auton Res. 1994;4(1-2):41-47.
- [CrossRef] [PubMed] [Google Scholar]
- Lower body negative pressure: physiological effects, applications, and implementation. Physiol Rev. 2019;99(01):807-851.
- [CrossRef] [PubMed] [Google Scholar]
- A simple test of cardiac function based upon the heart rate changes induced by the Valsalva maneuver. Am J Cardiol. 1966;18(01):90-99.
- [CrossRef] [PubMed] [Google Scholar]
- Physiology of positive accelerations: methods of increasing the tolerance to positive accelerations. In: A Text Book of Aviation Physiology. London: Pergamon; 1965:661-663.
- [Google Scholar]
- The Valsalva maneuver-3 centuries later. Mayo Clin Proc. 2004;79(04):577-578.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of the Valsalva maneuver on cardiac hemodynamics and right to left shunt in patients with patent foramen ovale. Sci Rep. 2017;7:44280.
- [CrossRef] [PubMed] [Google Scholar]
- The Valsalva maneuver: a bedside “biomarker” for heart failure. Am J Med. 2006;119(02):117-122.
- [CrossRef] [PubMed] [Google Scholar]
- Validation of an automated bilateral feet cold pressor test. Int J Psychophysiol. 2018;124(02):62-70.
- [CrossRef] [PubMed] [Google Scholar]
- Enhanced stress response by a bilateral feet compared to a unilateral hand cold pressor test. Stress. 2015;18(05):589-596.
- [CrossRef] [PubMed] [Google Scholar]
- Contribution of sympathetic activation to coronary vasodilatation during the cold pressor test in healthy men: effect of ageing. J Physiol. 2013;591(11):2937-2947.
- [CrossRef] [PubMed] [Google Scholar]
- Neural and physiological responses to a cold pressor challenge in healthy adolescents. J Neurosci Res. 2013;91(12):1618-1627.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with blood pressure response to the cold pressor test: the GenSalt Study. Am J Hypertens. 2013;26(09):1132-1139.
- [CrossRef] [PubMed] [Google Scholar]
- Blood Pressure and Cardiovascular Control in Offspring of Hypertensive and Normotensive Parents from Large Homogeneous Omani Arab Pedigrees. PhD Dissertation 2008
- [Google Scholar]
- Impact of age and sex on neural cardiovascular responsiveness to cold pressor test in humans. Am J Physiol Regul Integr Comp Physiol. 2020;319(03):R288-R295.
- [CrossRef] [PubMed] [Google Scholar]
- Regulation of cardiac function during a cold pressor test in athletes and untrained subjects. Eur J Appl Physiol. 2007;101(01):75-79.
- [CrossRef] [PubMed] [Google Scholar]
- Abnormal sympathetic reactivity to the cold pressor test in overweight humans. Am J Hypertens. 2012;25(12):1236-1241.
- [CrossRef] [Google Scholar]
- Baroreflex modulation of muscle sympathetic nerve activity during cold pressor test in humans. Am J Physiol Heart Circ Physiol. 2002;282(05):H1717-H1723.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of sympathetic autonomic stress from the cold pressor test on left ventricular function in young healthy adults. Physiol Rep. 2019;7(02):e13985.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of the cold pressor test on cardiac autonomic control in normal subjects. Physiol Res. 2009;58(01):83-91.
- [CrossRef] [PubMed] [Google Scholar]
- Responses of muscle sympathetic nerve activity and cardiac output to the cold pressor test. Jpn J Physiol. 1992;42(02):239-252.
- [CrossRef] [PubMed] [Google Scholar]
- The cold pressor test: effects on sympathetic nerve activity in human muscle and skin nerve fascicles. Acta Physiol Scand. 1989;137(03):325-334.
- [CrossRef] [PubMed] [Google Scholar]
- Beta-adrenoceptor blockade and cardiovascular response to the cold pressor test. Indian J Physiol Pharmacol. 1986;30(01):1-10.
- [Google Scholar]
- Early sympathetic neural responses during a cold pressor test linked to pain perception. Clin Auton Res. 2021;31(02):215-224.
- [CrossRef] [PubMed] [Google Scholar]
- 23andMe Research Team. Validity of the cold pressor test and pain sensitivity questionnaire via online self-administration. PLoS One. 2020;15(04):e0231697.
- [CrossRef] [PubMed] [Google Scholar]
- Cold pressor test as a predictor of hypertension. Hypertension. 1984;6(03):301-306.
- [CrossRef] [PubMed] [Google Scholar]
- Blood pressure response to cold pressor test in siblings of hypertensives. Indian J Physiol Pharmacol. 2003;47(04):453-458.
- [Google Scholar]
- Reduced sympathoneural responses to the cold pressor test in individuals with essential hypertension and in those genetically predisposed to hypertension. No support for the “pressor reactor” hypothesis of hypertension development. Am J Hypertens. 2004;17(10):863-868.
- [CrossRef] [Google Scholar]
- Cold pressor test in spinal cord injury-revisited. Spinal Cord. 2018;56(06):528-537.
- [CrossRef] [PubMed] [Google Scholar]
- Sympathetic neural responses to mental stress: responders, nonresponders and sex differences. Am J Physiol Heart Circ Physiol. 2009;296(03):H847-H853.
- [CrossRef] [PubMed] [Google Scholar]
- Hemodynamic and endocrine responsiveness to mental arithmetic task and mirror drawing test in patients with essential hypertension. Am J Hypertens. 1997;10(03):243-249.
- [CrossRef] [PubMed] [Google Scholar]
- Brain activation during addition and subtraction tasks in-noise and in-quiet. Malays J Med Sci. 2011;18(02):3-15.
- [Google Scholar]
- Mental arithmetic is a useful diagnostic evaluation in white coat hypertension. Am J Hypertens. 1998;11(1 Pt 1):41-45.
- [CrossRef] [PubMed] [Google Scholar]
- Short-term reproducibility of a mental arithmetic stress test. Clin Sci (Lond). 1991;81(05):593-601.
- [CrossRef] [PubMed] [Google Scholar]
- Mental arithmetic stress testing in patients with coronary artery disease. Am Heart J. 1984;108(01):56-63.
- [CrossRef] [PubMed] [Google Scholar]



