
Translate this page into:
Case of congenital mandibular malformation: A rarity
* Corresponding author: Dr. Dharmeshwar Arumugham, MDS, Department of Oral Medicine & Radiology, Tamil Nadu Government Dental College & Hospital (Affiliated to Tamil Nadu Dr. M.G.R. Medical University), Chennai, Tamil Nadu, India. adharmeshwar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Arumugham D, Sadaksharam J, Jayaram V. Case of congenital mandibular malformation: A rarity. Ann Natl Acad Med Sci (India) 2025;61:36-9. doi: 10.25259/ANAMS_20_2024
Abstract
The condition known as craniofacial duplication, or Diprosopus, is an exceedingly rare occurrence. The term “Diprosopus” originates from Greek, meaning “two-faced person.” This condition can involve a wide range of anomalies, from complete duplication of facial features to partial duplication of specific facial structures. It is a congenital developmental abnormality typically identified during prenatal development or in the early stages of a child’s growth. Formerly, it was believed to be an anomaly rather than a teratoma. The first documented report of this unique phenomenon was by Mclaughlin in 1948, and it was also recognized as a form of conjoined twinning. The classification system for this condition is based on the specific structures that exhibit duplication, resulting in four distinct types. Notably, this report discusses an extraordinary case involving the irregular growth of the mandible in a seven-year-old girl. This case is marked by the growth of an accessory structure stemming from the lower border of the mandible and is associated with developing tooth buds. The report delves into the diagnosis and management of such a unique and complex case.
Keywords
Congenital mandibular defect
Craniofacial duplication
Diprosopus
Mandible duplication

INTRODUCTION
Diprosopus is the term used to describe craniofacial duplication. Diprosopus is a term with Greek roots meaning “two-faced person.” It is an extremely rare congenital malformation where there is partial or complete duplication of the face with normal limbs and trunk. Diprosopus is considered one of the rarest forms of conjoined twins. Literature suggests an incidence of 1 in 180,000 births.1 The majority of diprosopic newborns with full duplication and single, normal limbs have significant central nervous system abnormalities.2 The majority of newborns with incomplete diprosopus (duplication of the maxilla, mandible, or mouth cavity) have a normal central nervous system. In these youngsters, the duplicated portions are removed to restore a natural look. It was first described by McLaughlin in 1948. A child with hemimandible duplication is discussed in this case report.3
CASE REPORT
The Department of Oral Medicine and Radiology received a seven-year-old female patient accompanied by her parents. The patient’s primary complaint was a painless swelling in the lower left side of her face that had been present for the past four years, leading to a disfigurement of the face. According to the patient’s mother, she had noticed a small swelling in the left lower side of her daughter’s face four years ago, which gradually increased in size over time. The swelling is now at its present size. The patient did not experience any pain associated with the swelling.
The mother provided a history of small tissue growth with discharge on the left lower side of her daughter’s face at seven months of age [Figure 1], which was initially diagnosed as a teratoma on the left chin. Subsequently, the growth was excised, resulting in a scar along the left lower border of the mandible. The histopathological examination of the excised specimen revealed it to be a congenital sinus.

- Congenital sinus tract aged seven months (yellow circle).
During the extraoral examination [Figure 2a-b], facial asymmetry was observed due to a swelling in the left lower third of face. The swelling was diffuse, measuring approximately 3 × 2 cm in the left body of the mandible region. The swelling extended from the left parasymphysis region to the left angle of the mandible region anteroposteriorly and from the inferior border of the mandible extending into the left submandibular region superoinferiorly. There was a surgical scar present on the skin over the swelling. Upon palpation, the swelling was found to be bony hard in consistency, non-tender, roughly ovoid, noncompressible, and fixed. There were no visible pulsations. On intraoral examination [Figure 2c], no abnormalities were noted. The history and clinical presentation suggested a benign lesion of the bone. Exostosis of the mandible and osteoma of the mandibles were considered for clinical differential diagnosis.
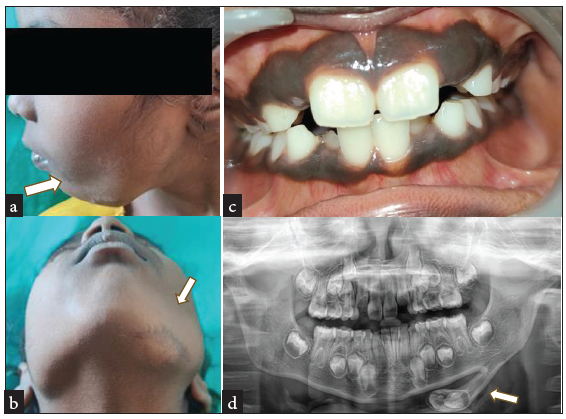
- (a and b) White arrow showing Diffuse extraoral swelling in the left lower border of mandible with surgical scar, (c) Intraoral view showing no abnormalities, and (d) White arrow in orthopantomogram showing extraosseous bony growth with enclosed tooth buds.
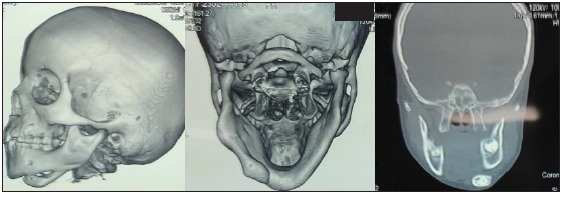
The ultrasonogram displayed a well-defined hyperechoic solid lesion measuring 11 × 6 mm near the left ramus of the mandible. The orthopantomogram [Figure 2d] revealed a radiopaque structure extending from the left lower border of the mandible to the angle region. This structure featured dense radiopaque formations, resembling developing tooth buds surrounded by radiolucent follicle space. The lateral skull view depicted a bone outgrowth from the left lower border of the mandible in the angle region. Computed tomography of facial bones [Figure 3] displayed that the posterior part of the outgrowth was attached to the lower border of the mandible in the angle region, while the anterior end was unattached and separate from the lower border of the mandible. The Hounsfield unit of the outer bone was similar to cortical bone, while that of the tooth bud-like structures enclosed within it was similar to enamel and dentin. Cone beam computed tomography [Figure 4] revealed an outgrowth measuring about 40 mm in length and 12 mm in maximum diameter originating from the lower border of the mandible at a point 8 mm beneath the tooth bud of 37. The developing supernumerary teeth consisted of enamel, dentin, and pulp space with incomplete root formation enclosed by a follicle. In addition, an accessory nerve/vascular bundle was evident at the junction of the outgrowth and the lower border of the mandible.
- Intraoral examination shows no abnormalities.
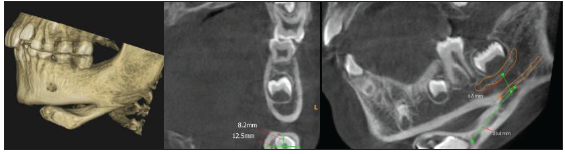
- Cone beam computed tomography showing accessory neurovascular bundle.
Clinical and radiographic features suggested a diagnosis of incomplete duplication of left hemimandible.
Surgical resection followed by recontouring was performed under general anesthesia.
Histopathologic examination [Figure 5] of the H and E stained section of the resected specimen demonstrates normal bone with minimal marrow spaces and dentinal tubules, which correlates with the finding of normal bone and tooth bud that was appreciated radiographically.
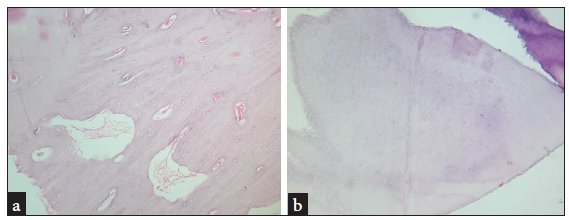
- (a) Normal bone with marrow spaces; (b) Dentinal tubules. Histopathologic photomicrograph (a,b: Hematoxylin and Eosin stained section under 10x magnification).
Postoperative [Figure 6] recovery was uneventful. The two-month follow-up revealed normal wound healing without any pain or paresthesia.

- (a) Postoperative images; (b) Postoperative orthopantomogram.
DISCUSSION
Diprosopus is a rare condition that can encompass a wide range of congenital anomalies, including complete duplication of facial features or partial duplication of facial structures. Studies have shown a 2:1 female-to-male ratio, indicating a higher prevalence in females.4 In cases of partial duplication, the maxilla, mandible, or oral cavity are commonly affected. Partial duplication of individual mandibular structures or symmetric double mandibular arches is a common manifestation. These duplicated mandibles may include the accessory condyle, coronoid process, mandibular body, and the canal. Supernumerary teeth are often present, typically in regular tooth shapes, and may be impacted or erupt into functional occlusion.
The pathogenesis of craniofacial duplication remains poorly understood. Various reasons have been attributed to mandibular duplication5:
Duplication of first brachial arch
Sequestration of totipotent stem cells resulting in developmental anomalies
Split notochord syndrome
Mandibular growth center duplication around the margins of the stomatodeal plate
Amniotic band syndrome
Beatty proposed a hypothesis that partial oral duplication can occur due to developmental excess. He reported a case with accessory mouth. His idea proposes that an auxiliary growth center forms in the regular mandibular process, eventually developing into an accessory mandible and mouth.6
Mason Barr identified three forms of facial duplication in 19824:
Eye and nose duplication, including maxillary or mandible duplication
Nasal or maxillary duplication
Maxillary duplication which may or may not include mandible and pituitary duplication; he described pituitary duplication in isolation but was unsure about the presence of isolated mandibular duplication
In 1989, Chen and Noordhoff 7 suggested a technique for classifying stomodeal formations. This was based on the abnormalities seen in the actual mouth, the degree of development of the duplicated lip or jaw, and their location and components:
Type I (duplicated mouth)
Type II (duplication of the maxilla upper lip or mandible lower lip complex)
Type III (centrally located, poorly developed lip-jaw duplication)
Bhuyan et al.1 proposed a categorization approach that focuses on oral duplication in 1990:
Maxillary duplication with normal mouth
Rudimentary mandible with duplicated mouth
Partial duplication of the mandible with a single mouth
Anencephaly accompanying diprosopus
An additional jaw should be differentiated from a teratoma with osseous toothlike features. Teratomas are encapsulated tumors that contain tissue or organ components derived from three germ layers.
In the case of a duplicated mandible, the accessory structures are well organized, whereas in a teratoma, they are arranged haphazardly. Supernumerary teeth may be found in duplicated jaws. The shapes of these supernumerary teeth associated with diprosopus were found to be normal.8
The treatment of choice is surgical resection and recontouring with good cosmetic and functional results.
CONCLUSION
Diprosopus is an exceptionally rare condition that can result in significant cosmetic and functional challenges. It can manifest as partial duplication, involving a single bone or a portion of a bone, or as complete duplication. Additionally, some reported cases have indicated the presence of facial cleft or parotid aplasia alongside mandibular duplication. Surgical resection and recontouring have emerged as highly effective interventions, yielding positive outcomes in addressing these complexities.
Acknowledgments
The authors sincerely acknowledge the departments for their support: Department of Oral and Maxillofacial Surgery and Department of Oral Pathology and Microbiology.
Authors’ contributions
DA, JS: Manuscript preparation; JS, VJ: Drafting and revising of manuscript.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Diprosopus a rare craniofacial malformation. Asian J Neurosurg. 2018;13:1257-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Partial duplication of the jaw: Case reports and review of relevant publications. Br J Oral Maxillofac Surg. 2020;58:34-42.
- [CrossRef] [PubMed] [Google Scholar]
- Duplication of the Mandible: Plastic and Reconstructive Surgery. Available from: https://journals.lww.com/plasreconsurg/citation/1979/07000/duplication_of_the_mandible.28.aspx [Last accessed 2024 Jun 5].
- Facial duplication: Case, review, and embryogenesis. Teratology. 1982;25:153-9.
- [CrossRef] [PubMed] [Google Scholar]
- Partial duplication of the mandible, parotid aplasia and facial cleft: A rare developmental disorder. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116:e202-9.
- [CrossRef] [PubMed] [Google Scholar]
- Diprosopus: A unique case and review of the literature. Teratology. 2002;66:282-7.
- [CrossRef] [PubMed] [Google Scholar]
- Duplication of stomatodeal structures: Report of three cases with literature review and suggestion for classification. Plast Reconstr Surg. 1989;84:733-40.
- [PubMed] [Google Scholar]
- Duplication of the oral cavity and mandible: A rare congenital craniofacial anomaly. BMJ Case Rep. 2020;13:e233799.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]



