
Translate this page into:
Dentigerous Cyst in the Maxillary Anterior Region of a Pediatric Patient
Address for correspondence Nivethitha Nagarajan, BDS, Department of Oral Medicine and Radiology, Tamil Nadu Government Dental College and Hospital Chennai, Chennai, Tamil Nadu 600003, India (e-mail: nive_revathi@yahoo.co.in).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Dentigerous cyst is a common type of odontogenic cyst of the oral and maxillofacial region. It commonly occurs in the second or third decades and rare cases appear in the first decade of age. It is a developmental cyst associated with unerupted/impacted tooth. Radiographically, it appears as unilocular, radiolucent area along the cementoenamel junction of the associated tooth. Larger dentigerous cysts may be treated with marsupialization, and smaller dentigerous cysts are treated with enucleation of the cyst and extraction of the associated tooth. This case report presents a case of dentigerous cyst in the right maxillary region in a young child and was diagnosed using radiographs and removed by surgical excision.
Keywords
dentigerous cyst
enucleation
maxilla
radiolucent
squamous epithelium
unerupted tooth

Introduction
Dentigerous cysts are cystic lesions in the oral and maxillofacial area radiographically represented by a well-defined unilocular radiolucent area usually involving an impacted tooth crown. It is considered as the most common type of odontogenic cyst at approximately 20% of all jaw cysts. It is mainly associated with the mandibular third molar, maxillary third molar and maxillary canines, with peak incidence in the second and third decades.1 The occurrence of this cyst in the first decade is relatively low at approximately 4 to 7%. Histologically, they are represented by a cavity lined by the nonkeratinizing thin epithelium without rete pegs.2 These cysts are usually asymptomatic and are detected by routine radiographic examination. The removal of the cystic lesion and the extraction of the unerupted tooth is the main treatment to prevent the recurrence of the cystic lesion.3 This case report presents a case of dentigerous cyst in the right maxillary region in a young child and was diagnosed using radiographs and removed by surgical excision.
Case Report
A 7-year-old male reported to the department of oral medicine and radiology with the chief complaint of swelling in the upper right front region of the jaw and delayed eruption of upper front tooth for the past 2 months but not associated with pain. History revealed that the swelling was insidious in onset, which gradually increased and attained the present size. There was no history of fever, trauma, bleeding or pus discharge related with the swelling. The past medical and family history was not contributory.
On general examination, the patient appeared moderately built and nourished. On extraoral examination mild facial asymmetry in the right maxillary region was observed. On palpation, the swelling was firm to hard in consistency, nontender, fixed to the underlying bone, free from the overlying skin, and with no tenderness or secondary changes. Intraorally, a solitary swelling was present in the right maxillary labial gingival and labial vestibular region, measuring approximately 2.0 × 2.0 cm, extending superiorly from the labial vestibular region and inferiorly to the marginal gingival region in relation to the right maxillary central incisor (11) and lateral incisor (12). The swelling appears to extend till the palatal gingival region in the right maxillary incisors. The surface of the lesion appeared smooth with diffuse borders and no secondary changes like bleeding or pus discharge present (►Fig. 1A, B). On palpation, swelling was nontender, noncompressible, nonpulsatile, not depressible, and hard in consistency with expansion of labial and palatal cortical regions.

- Intraoral preoperative photograph of the lesion (A, B). Preoperative maxillary occlusal radiograph (C) and orthopantomogram (D). White arrows indicate the lesion.
The patient's consent was obtained and the radiographical examination was performed. Radiological examination was performed using maxillary occlusal radiograph, and orthopantomogram revealed a well-defined radiolucent area approximately 2.0 × 2.0 cm with well-defined radiopaque borders in the posterior region in relation to 11, 12, 13, 14, 52 and 53.
There was displacement of permanent and deciduous right maxillary incisors (11,12, 13, 52 and 53) and the radiolucency was laterally along the tooth root, partially surrounding the crown suggestive of the lateral variety. There was no root resorption and the surrounding bone appeared normal. Orthopantomogram reveals erupting permanent premolars, first molars, second molars, and developing third molars. The biochemical and microbiological investigations were within normal limits (►Fig. 1C-D).
Complete surgical excision of the lesion was done under local anesthesia. Teeth (52, 53 and 11) were extracted as on surgical exposure, the roots were completely contained in the lesion (►Fig. 2A). The permanent maxillary incisor was extracted, as the tooth was completely contained inside the lesion. Gross examination of the specimen showed gray white cystic soft-tissue fragments (►Fig. 2C). Histopathological examination revealed lesion lined by stratified squamous epithelium with ulceration, and stroma showed collections of inflammatory infiltrate composed of lymphocytes and plasma cells, congested by blood vessels with focal myxoid change and hemorrhage. Bony spicules were seen (►Fig. 2B).

- Intraoperative photograph of the lesion (A) and the excised lesion along with the extracted teeth (B). Photograph of histopathological section, revealing lesion lined by stratified squamous epithelium with ulceration, and stroma showing collections of inflammatory infiltrate composed of lymphocytes and plasma cells, congested by blood vessels with focal myxoid change and areas of hemorrhage (C).
The overall clinical, radiologic and histopathological diagnosis confirmed the final diagnosis of dentigerous cyst. The follow-up occlusal radiograph was taken by the second month, which showed no recurrence of the lesion at the site (►Fig. 3C) The patient is under regular follow-up for the past 1 year, the eruption pattern of other teeth appears normal, and the rehabilitation will be done when the adjacent permanent teeth erupt and bone growth is adequate (►Fig. 3A-B).

- Immediate postoperative photograph of the lesion (A) 3-month follow-up photograph (B). 3-month postoperative maxillary occlusal radiograph (C).
Discussion
Dentigerous cyst is a type of odontogenic cyst that encloses the crown of an unerupted tooth by expansion of the follicle and is commonly attached to the neck of the involved tooth. The term dentigerous is preferred, the literal meaning being “tooth bearing.”4 Dentigerous cysts are usually asymptomatic, with the majority of small cysts identified incidentally through routine radiographic examination or occasionally from delay in the eruption of a permanent tooth.5 The average age of children who develop the dentigerous cysts is 11.05 years. This is the age in which the permanent canines and premolars have their greatest eruptive potential and the widening of dental follicle is a part of the eruptive process.6 Dentigerous cysts in the pediatric group commonly occur in the late mixed dentition period, as there is increased probability of impaction of the maxillary canines and of periapical inflammation from a nonvital deciduous tooth spreading to involve the follicle of an unerupted permanent succedaneous tooth.
Two types of dentigerous cysts have been described according to the etiopathogenesis.
Developmental and inflammatory types. The developmental type is the most common type, which usually surrounds the crown of an unerupted tooth by fluid accumulation between the layers of the enamel organ.7 The inflammatory type of dentigerous cyst is usually associated with the roots of a nonvital primary tooth.8 Three types of dentigerous cyst have been radiographically described by Thoma-Robinson-Bernier: The central variety, in which the radiolucency surrounds just the crown of the tooth, with the crown projecting into the cyst lumen. In the lateral variety, the cyst develops laterally along the tooth root and partially surrounds the crown, and the circumferential variant exists where the cyst surrounds the crown and extends down along the root9 (►Fig. 4A,B,C).
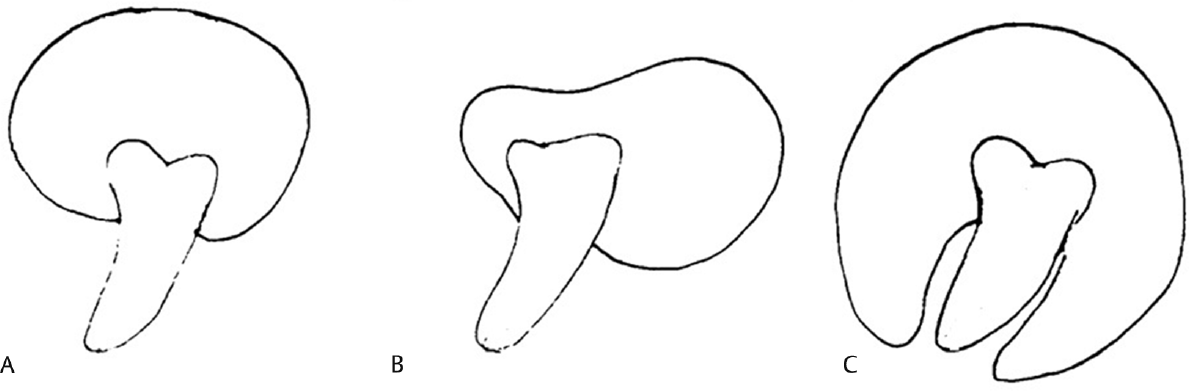
- The central variety, in which the radiolucency surrounds just the crown of the tooth, with the crown projecting into the cyst lumen (A). In the lateral variety, the cyst develops laterally along the tooth root and partially surrounds the crown, (B) and the circumferential variant exists where the cyst surrounds the crown and extends down along the root (C).
It is commonly associated with impacted, unerupted, embedded tooth, odontome or supernumerary tooth. Large odontoma can cause a delay in the eruption of permanent teeth and can further develop cystic lesions as dentigerous cysts.10 The clinical examination reveals a missing tooth or teeth and possibly a hard swelling, occasionally resulting in facial asymmetry with no pain or discomfort.11 Delayed tooth eruption of the involved tooth is also a common presentation. Bilateral and multiple cysts have been reported in patients with syndromes such as basal cell nevus syndrome, mucopolysaccharidosis, cleidocranial dysplasia, and prolonged concurrent use of cyclosporine and calcium channel blockers.12,13 The dentigerous cyst is potentially capable of becoming an aggressive lesion. Expansion of the bone with facial asymmetry, displacement of teeth, severe root resorption of the adjacent teeth, and pain are possible sequelae brought about by continued enlargement of the cyst.14 Cystic involvement of the unerupted mandibular third molar usually results in a “hollowing-out” of the ramus, extending up to coronoid process and condylar process, and expansion of the cortical plate due to the pressure exerted by the lesion.14
Radiographically, the cyst presents as a well-defined unilocular radiolucency, often with sclerotic border. Since the epithelial lining is derived from the reduced enamel epithelium, this radiolucency typically surrounds the crown of the tooth.9 If the follicular space on radiograph is more than 5 mm, an odontogenic cyst can be suspected. Other odontogenic cysts like radicular cysts, odontogenic keratocysts, and odontogenic tumors such as ameloblastoma, Pindborg tumor, odontoma, odontogenic fibroma, and cementomas may share the same radiologic features as dentigerous cysts.12 A large dentigerous cyst may be multilocular in radiological appearance because of the persistence of bone trabeculae within the radiolucent area.
The dentigerous cyst is normally lined with nonkeratinized stratified squamous epithelium and filled with clear, amber-colored fluid that not infrequently is rich in cholesterol and cholesterol esters.15 Rete peg formation is usually absent except in cases which are secondarily infected. The connective tissue wall is thickened and composed of a loose fibrous connective tissue or sparsely collagenized myxomatous tissue.14 As the lining is derived from reduced enamel epithelium, it is generally 2 to 4 cell layer thick primitive type.9 The impacted tooth exerts a pressure on follicle, which obstructs the venous outflow and induces a rapid transudation of serum across capillary walls. The increased hydrostatic pressure exerted by pooling of this fluid causes separation of crown from follicle with or without the reduced enamel epithelium. The osmolality of the cystic fluid is modified by the increased permeability to glycosaminoglycans like hyaluronic acid, heparin and chondroitin sulfate, which cause expansile growth rapidly.16
The treatment modality is indicated in each individual case, such as cyst size and site, patient age, the dentition involved, and the involvement of vital structures. Cyst enucleation without extraction of the impaction, and decompression are two treatment modalities indicated in growing children and adolescents to salvage the involved dentition.17 In extensive lesion, surgery or marsupialization is commonly recommended for dentigerous cysts, because they often block eruption of teeth, become large, displace teeth, destroy bone, encroach on vital structures and, occasionally even, lead to pathologic fracture.18 Rarely, dentigerous cyst transforms to oral squamous cell carcinoma, ameloblastoma or mucoepidermoid carcinoma in the adult population if the cyst in untreated for a longer period of time.
Conclusion
Dentigerous cyst is the second common odontogenic cyst in the oral and maxillofacial region. The prognosis of the cyst is good, and recurrence is rare with regular follow-up. Although these cysts are rare in the first decade, they can develop in the early stages of life, and cause interference in tooth development and eruption pattern. Hence, early clinical, histopathological diagnosis and complete excision of the lesion with long-term follow-up is required to prevent occurrence of destructive lesions.
Acknowledgment
The authors wish to thank Department of General Pathology, Madras Medical College, for providing histopathological aspects. Department of Oral and Maxillofacial Surgery, Tamil Nadu Government Dental College and Hospital, for providing the surgical aspects.
Conflict of Interest
None declared.
References
- Unusual imaging features of dentigerous cyst: a case report. Dent J (Basel). 2019;7(03):1-7.
- [CrossRef] [PubMed] [Google Scholar]
- Oral and Maxillofacial Pathology. 3rd ed. St. Louis, MO, USA: Saunders; 2008:678-740.
- [Google Scholar]
- Marsupialization: a conservative approach for treating dentigerous cyst in children in the mixed dentition. J Indian Soc Pedod Prev Dent. 2010;28(03):203-208.
- [CrossRef] [PubMed] [Google Scholar]
- The pathogenesis of odontogenic cysts: a review. J Oral Pathol. 1975;4(01):31-46.
- [CrossRef] [PubMed] [Google Scholar]
- Case report: preservation of teeth involved with an odontogenic cyst. Eur Arch Paediatr Dent. 2010;11(03):146-148.
- [CrossRef] [PubMed] [Google Scholar]
- Histological analysis of 41 dentigerous cysts in a paediatric population. J Oral Pathol Med. 2019;48(01):74-78.
- [CrossRef] [PubMed] [Google Scholar]
- Non syndromic unilateral dentigerous cyst in a 4-year-old child: A rare case report. Contemp Clin Dent. 2011;2(04):398-401.
- [CrossRef] [PubMed] [Google Scholar]
- Inflammatory dentigerous cysts of children treated by tooth extraction and decompression–report of four cases. Br Dent J. 1999;187(11):587-590.
- [CrossRef] [PubMed] [Google Scholar]
- An infected dentigerous cyst associated with an impacted permanent maxillary canine, inverted mesiodens and impacted supernumerary teeth. J Pharm Bioallied Sci. 2013;5(Suppl. 02):S135-S138.
- [CrossRef] [PubMed] [Google Scholar]
- Dilated odontoma: A report of two cases from a radiological perspective. Contemp Clin Dent. 2016;7(01):107-110.
- [CrossRef] [PubMed] [Google Scholar]
- Cysts and cyst like lesions of the jaws. In: Stuart CW, Michael JP. eds. Oral Radiology: Principles and Interpretation. St. Louis, MO: Elsevier; 2009:346-348.
- [Google Scholar]
- Bilateral maxillary dentigerous cysts: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95(05):632-635.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral mandibular cysts associated with cyclosporine use: a case report. Pediatr Nephrol. 2001;16(12):993-995.
- [CrossRef] [PubMed] [Google Scholar]
- Potentialities of oral epithelium manifest by mandibular dentigerous cysts. Oral Surg Oral Med Oral Pathol. 1957;10(03):271-284.
- [CrossRef] [PubMed] [Google Scholar]
- Pathogenesis of odontogenic cysts. In: Investigative Pathology of the Odontogenic Cyst. New Jersey: CRC Press Boca Raton; 1991:88-109.
- [Google Scholar]
- Management of extensive dentigerous cysts. Br Dent J. 2005;198(04):203-206.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical management of odontogenic cysts and tumors. In Peterson LJ, Indresano TA, Marciani RD, Roser SM. eds. Principles of Oral and Maxillofacial Surgery. Philadelphia: JB Lippincott; 1992:685-688.
- [Google Scholar]



