
Translate this page into:
Evaluation of Clinical, Demographic, and Biochemical Profiles of Trinidadian Patients Undergoing Coronary Angiography
 , Surapaneni Krishna Mohan5, Vishnu Priya6
, Surapaneni Krishna Mohan5, Vishnu Priya6
Address for correspondence Shivananda Nayak B, MSc, PhD, FAGE, FACB, NRCC-CC, FISBT, FABM, PGDCHC, DSc, Department of Preclinical Sciences, The University of the West Indies, Faculty of Medical Sciences Trinidad and Tobago, West Indies (e-mail: shiv25@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background
Trinidad and Tobago ranks number 45 in the world for total deaths due to coronary heart disease. Predictive tests for coronary angiographic results set the basis for earlier monitoring of the disease before additional complications become obvious.
Aims and Methods
This study aimed to evaluate the anthropometric and biochemical parameters of 124 patients with suspected coronary artery disease (CAD) in Trinidad and how these parameters correlate to the findings at angiography.
Results
The biochemical parameters showed statistically significant correlations with CAD severity by Spearman's rank-order correlation. Two clinical parameters showed significant associations with CAD severity—ethnicity (χ2 (4) = 12.925, p = 0.012) and presence of type 2 diabetes at baseline (χ2 (4) = 21.483, p < 0.001).
Conclusion
Biochemical parameters such as fasting blood sugar, N-terminal pro B-type natriuretic peptide, creatinine, and hemoglobin A1c were well correlated and well associated with the severity of CAD after diagnosis by the process of coronary angiography. Hence, these factors can be taken into consideration to predict the severity of CAD.
Keywords
coronary angiography
coronary artery disease
glycated hemoglobin
diabetes mellitus
NT-proBNP

Introduction
Coronary artery disease (CAD) has become the most common type of heart disease worldwide. It is the major cause of morbidity and mortality globally and has therefore become a major public health burden.1 CAD has caused substantial economic costs on the governments of various countries for monitoring and treatment.2 In Trinidad specifically, 21% of the population dies of cardiovascular causes annually, with heart disease being the number 1 cause of death. Trinidad and Tobago also ranks number 45 in the world for total deaths due to coronary heart disease.3 Despite the efforts of medical research and governments in reducing this health burden, recent trends have shown that the disease incidence has escalated and has started affecting a younger age group.4 A variety of tests can assist in the diagnosis of CAD electrocardiography, stress testing, echocardiography, chest X-rays, and laboratory blood tests. Coronary angiography is considered to be the “gold standard” for the diagnosis of CAD as it is used to identify the precise location and severity of the disease.5 It has also been acknowledged that in spite of successful treatment achievements in recent decades, the mortality of patients with heart disease continues to be elevated.6 Early detection and control of known and emerging risk factors of CAD will enable better monitoring of the disease at an earlier stage. Hence, further study of specific cardiac factors may be able to generate predictive tests for coronary angiographic results and set the basis for earlier monitoring of the disease before additional complications arise. This study aimed to examine various clinical, demographic, and biochemical profiles of Trinidadian patients undergoing coronary angiography and determine how they correlate to findings at angiography. The objective is to better target parameters related to CAD and its severity. Correlating such parameters with patients' angiographic results has not been conducted in Trinidad or the Caribbean region thus far. This study is therefore of much significance and is a vital step in assessing ways to diagnose and control CAD at an earlier stage.
Materials and Methods
Study Design and Setting
The research method was of a quantitative orientation, with the research design as experimental with patient questionnaires. As such, this research method emphasized measurements and the statistical analysis of the data collected through questionnaires or by manipulating preexisting numerical data to explain the phenomenon.
Study Participants and Sample Size
Since this was a quantitative research methodology, a sample size calculation was not followed. Sample size above the minimum requirement for statistical analysis was provided. One hundred and twenty-four (n = 124) patients age range 17 to 70 years were included in this study. All patients were required to fast for 10 to 12 hours overnight. The included patients were referred for angiography at the catheterization laboratory of the Eric Williams Medical Sciences Complex hospital. This hospital was selected on the basis that it is centrally located in Trinidad and is the only public (government funded) cardiac catheterization laboratory in the island. Its referral base for cardiac catheterization is unselected and comes from the entire country's public health network. The patient pool therefore is representative of most of the country's population and was not possible to be controlled by the authors. The protocol for the study was approved by the Ethics Committee of the Faculty of Medical Sciences, The University of the West Indies, Ref: CEC107/12/15.
Collection of Clinical and Biochemical Data
After getting informed consent, patient age, self-reported ethnicity, smoking status, diet, medical history, and family history were collected by administering the questionnaire to the study participants. Blood pressure, waist and hip circumferences, and body weight were measured using standard procedures. Measurement of the waist and hip circumferences was obtained using a tape measure: the patient was first asked to stand upright with arms relaxed at their sides, feet evenly spread apart at approximately shoulder width, and body weight evenly distributed. The waist measurement was made at the midpoint between the top of the upper edge of the pelvic bone and the lowest point of the ribcage that can be palpated. Once this location was obtained, the tape measure was wrapped snugly around the body ensuring that the abdominal muscles were relaxed. For hip circumference, the tape measure was wrapped around the hips at the widest circumference of the buttocks. The patients' weights in kilograms were measured using a medical scale and heights were obtained in meters using a stadiometer.
The 10 mL of fasting blood sample was collected from each patient and further used to analyze fasting blood sugar (FBS) (sodium fluoride/potassium oxalate tube), lipid profile, creatinine, uric acid, interleukin-6, insulin, creatine kinase, creatine kinase MB izoenzyne, N-terminal pro B-type natriuretic peptide (NT-proBNP), and soluble ST2. All these parameters were analyzed on an automated dry multichannel analyzer, except for soluble ST2, which was analyzed using Presage ST2 Assay Elisa Kit due to equipment and resource availability. Interleukin-6, insulin, and NT-proBNP were analyzed using the Cobas e601 machine and the other parameters were measured using the Vitros 4600 analyzer. Whole blood obtained from the K2EDTA tube was used to evaluate glycated hemoglobin using the Arkray A1c analyzer.
Coronary Angiographic Assessment
Patients were grouped according to the severity of CAD after undergoing coronary angiography. These patients were grouped as having no CAD, mild or nonobstructive CAD, single-vessel disease (SVD), double-vessel disease (DVD), and triple-vessel disease (TVD), according to the number of vessels involved and the degree of stenosis. Stenosis of a vessel was characterized as significant once the vessel was more than or equal to 50% narrowed. CAD was therefore defined as 50% or more reduction in the luminal diameter by obstruction in one or more coronary arteries as assessed by using angiography by a cardiologist. The cardiologist then suggested the appropriate revascularization strategy (percutaneous coronary intervention or coronary artery bypass grafting) to be performed or optimal medical therapy to treat the patient.
Statistical Analysis
Statistical analyses were performed using SigmaPlot 11 and IBM SPSS Statistics 20. Normally distributed data were presented as mean ± standard deviation, whereas data with nonnormal distributions were expressed as median (interquartile range). Categorical data were presented as percentages and coded before statistical analysis. The presence of CAD was coded as 1 and absence as 0. Additionally, severity of CAD was coded as follows: no disease—0, mild CAD—1, SVD—2, DVD—3, and TVD—4. Correlations between nonnormal parameters and CAD presence and severity were assessed using a nonparametric test: Spearman's rank-order correlation coefficient. Chi-square test was also used to compare the associations between categorical variables. Statistical significance was accepted when the p-value was less than 0.05. In addition to these tests, the eta coefficient of nonlinear association was evaluated between some of the intervals and categorical variables, that is, type 2 diabetes (T2D) at baseline and coronary angiography severity, and between alcohol status and CAD severity, to further support the previous results obtained. Finally, multinomial logistic regression was conducted to show the significant predictors of CAD presence and severity after adjustment for possible confounding factors.
Results
Baseline Characteristics
►Table 1 depicts the baseline descriptive characteristics of the patients analyzed in this study.
| Characteristic | Cohort (n = 124) |
|---|---|
| Age (y) | 56 ± 11 |
| Male | 78 (62.9%) |
| Female | 46 (37.1%) |
| Systolic blood pressure (mm Hg), median | 135 |
| Diastolic blood pressure (mm Hg), median | 80 |
| Body mass index (kg/m2), median | 27 |
| Waist:hip, median | 0.94 |
| Smokers | 27 (21.8%) |
| Alcoholics | 12 (9.7%) |
| Diet | |
| Omnivorous | 111 (89.5%) |
| Vegetarian | 13 (10.5%) |
| Family history | |
| Heart disease | 80 (64.5%) |
| Diabetes mellitus | 73 (58.9%) |
| Stroke | 24 (19.4%) |
| Self-reported ethnicity | |
| Indo-Trinidadians | 93 (75%) |
| Afro-Trinidadians | 19 (15.3%) |
| Others (mixed) | 12 (9.7%) |
| Chronic conditions before angiography | |
| STEMI | 18 (14.5%) |
| NSTEMI | 23 (18.5%) |
| Hypertension | 80 (64.5%) |
| Hyperlipidemia | 65 (52.4%) |
| Type 2 diabetes | 59 (47.6%) |
Abbreviations: NSTEMI, non-ST-elevation myocardial infarction; STEMI, ST-elevation myocardial infarction.
The number of patients falling into each category of CAD normal (9.7%), mild CAD (18.5%), SVD (26.6%), DVD (15.3%), and TVD (29.9%) were categorized. It was observed that out of 124 patients, most were males. Majority of these patients were of East Indian descent (Indo-Trinidadians) with an omnivorous diet and hypertensive at baseline.
Correlations between the clinical and biochemical parameters with the presence and severity of CAD were analyzed. Among the parameters analyzed, age, FBS, NT-proBNP, and hemoglobin A1c (HbA1c) showed strongly positive statistically significant relationships with CAD (p < 0.001). There was a moderately positive correlation with creatinine (p = 0.006) as shown in ►Table 2. These positive correlations suggest that as both of these parameters, NT-proBNP and HbA1c, increased in the blood, it was likely that the severity of CAD would increase, from no disease to TVD. There was no statistically significant relationship between soluble ST2 and CAD severity (r = 0.029, p = 0.745).
| Parameter | Cohort (n = 124) | Correlation coefficient | p-Value |
|---|---|---|---|
| Age (y) | 56 ± 11 | 0.387 | <0.001 |
| Systolic blood pressure (mm Hg) | 135 (30.8) | 0.141 | 0.119 |
| Diastolic blood pressure (mm Hg) | 80 (17) | −0.069 | 0.446 |
| Waist:hip | 0.94 (0.1) | 0.126 | 0.165 |
| Body mass index (kg/m2) | 26.7 (7.4) | −0.063 | 0.490 |
| FBS (mg/dL) | 97 (37.5) | 0.418 | <0.001 |
| Trigs (mg/dL) | 2.1 ± 0.19 | 0.150 | 0.097 |
| HDL (mg/dL) | 1.6 ± 0.13 | −0.157 | 0.082 |
| LDL (mg/dL) | 81 (70.5) | 0.158 | 0.080 |
| TC (mg/dL) | 2.2 ± 0.15 | 0.133 | 0.142 |
| CK (mg/dL) | 1.9 ± 0.31 | −0.136 | 0.133 |
| CKMB (mg/dL) | 12 (8) | 0.077 | 0.393 |
| Creatinine (mg/dL) | 1 (0.36) | 0.244 | 0.006 |
| Uric acid (mg/dL) | 5.7 (2.3) | 0.099 | 0.274 |
| IL-6 (pg/mL) | 4.5 (19.2) | 0.095 | 0.295 |
| NT-proBNP (pg/mL) | 2.4 ± 0.8 | 0.307 | 0.001 |
| Soluble ST2 (ng/mL) | 30.3 (28) | 0.029 | 0.745 |
| IR (HOMA) | 4.2 (3.6) | 0.078 | 0.388 |
| HbA1c (%) | 6.1 (1.4) | 0.488 | <0.001 |
Abbreviations: CAD, coronary artery disease; CK, creatine kinase; FBS, fasting blood sugar; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HOMA, homeostatic model assessment; IL, interleukin; IR, insulin resistance; LDL, low-density lipoprotein; NT-proBNP, N-terminal pro B-type natriuretic peptide; TC, total cholesterol; Trigs, triglycerides.
►Table 3 reveals the results of the chi-square test association between categorical clinical variables and CAD presence and severity. A statistically significant relationship between gender and presence of CAD (χ2 (1) = 4.978, p = 0.026) with an odds ratio of 3.895 at 95% confidence interval (1.102, 13.763) was observed suggesting that CAD is approximately four times more likely to be present in males than females. A statistically significant relationship was also found between male gender and CAD severity (χ2 (4) =11.894, p = 0.018).
| Parameter | Cohort (n = 124) | With CAD presence | With CAD severity | |||
|---|---|---|---|---|---|---|
| Chi-square | p-Value | OR (95% CI) | Chi-square | p-Value | ||
| Gender—male | 78 (62.9%) | (1) = 4.978 | 0.026 | 3.895 (1.102, 13.763) | (4) = 11.894 | 0.018 |
| T2DM presence (at baseline) | 59 (47.6%) | (1) = 5.091 | 0.024 | 5.182 (1.086, 9.548) | (4) = 21.483 | <0.001 |
| Ethnicity (Indo-Trinidadians) | 93 (75%) | (1) = 4.429 | 0.072 | 3.480 (1.032, 11.739) | (4) = 12.925 | 0.012 |
Abbreviations: CAD, coronary artery disease; CI, confidence interval; OR, odds ratio; T2DM, type 2 diabetes mellitus.
An association was also observed between the presence of T2D before angiography and the presence of CAD with statistical significance (χ2 (1) = 5.091, p = 0.024) and an odds ratio of 5.182 at 95% confidence interval (1.086, 9.548). This indicated that the odds of a patient with T2D presenting with CAD is 5.182 times more likely than individuals without T2D. A statistically significant relationship was also observed between presence of T2D at baseline and the severity of CAD (χ2 (4) = 21.483, p < 0.001).
No statistically significant associations were established between smoking and alcohol consumption with the presence and severity of CAD. None was also observed between the presence of hypertension and hyperlipidemia at baseline with the presence or severity of CAD.
Indo-Trinidadians formed 75% of this cohort of patients. Ethnicity, represented as Indo-Trinidadians or not (mixed and Afro-Trinidadians), was found to have a statistically significant correlation with CAD severity (χ2 (4) = 12.925, p = 0.012). The relationship between CAD severity and number of patients of the various ethnic groups is shown in ►Fig. 1.
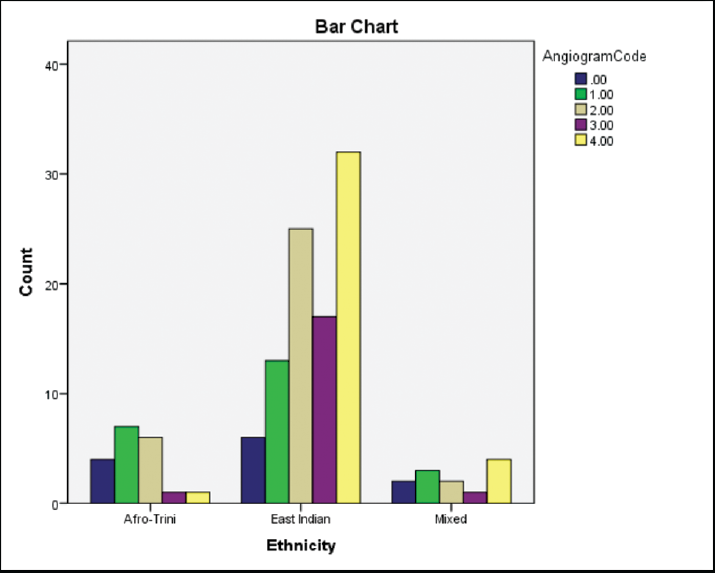
- Relationship between coronary artery disease severity and number of patients of the various ethnic groups.
Another test was performed to confirm these results, called the eta measure which is part of an analysis of variance test. This found moderate associations with these same categorical variables—T2D presence at baseline and ethnicity with CAD severity. The presence of T2D before coronary angiography resulted in an eta value of 0.413 (eta2 = 0.171) and ethnicity (Indo-Trinidadian/not Indo-Trinidadian) presented an eta value of 0.300 (eta2 = 0.09). When ethnicity was categorized as Indo-Trinidadian, Afro-Trinidadian, and other (mixed), a moderately strong association was also found, with an eta value of 0.333 (eta2 = 0.111) (not shown in the table).
Another regression was performed using gender, smoking status, alcohol consumption, and ethnicity as possible confounders with CAD severity and the biochemical parameters. The results of this regression showed that age, FBS, interleukin-6, and NT-proBNP were all significant predictors of the severity of CAD (►Table 4).
| Parameter | p-Value | Exp (B) (95% CI) | |
|---|---|---|---|
| Before | After | ||
| Age | 0.037 | 0.009 | 0.851 (0.753, 0.961) |
| FBS | 0.004 | 0.042 | 0.910 (0.832, 0.996) |
| IL-6 | 0.009 | 0.005 | 1.126 (1.037, 1.224) |
| NT-proBNP | 0.068 | 0.038 | 0.998 (0.997, 1.000) |
Abbreviations: CI, confidence interval; FBS, fasting blood sugar; IL, interleukin; NT-proBNP, N-terminal pro B-type natriuretic peptide.
Discussion
The focus of this study was to evaluate the anthropometric and biochemical parameters and to determine how these parameters correlated to the findings of coronary angiography. Angiographic findings were grouped by the number of diseased coronary vessels and the percentage of coronary stenosis. The results observed were statistically significant correlations between the severity of CAD and age, FBS, glycated hemoglobin, creatinine, and NT-proBNP levels.
A more refined approach to risk assessment may include the use of additional biological markers of pathophysiological processes, for example, those of myocardial fibrosis and stretch. An enhanced risk assessment would therefore be of significant clinical value to precisely identify heart failure patients who are at risk of death. These patients could therefore be targeted for more intensive treatment and monitoring at earlier stages. In addition to the already-established risk factors of CAD, a few emerging parameters were incorporated into the study to enhance the risk assessment of the patient. The early identification and treatment of these risk factors will therefore aid in accelerating disease monitoring and prevention and in turn improve the morbidity rate.
Glycemic control is a known risk factor associated with both the presence and severity of CAD as supported by the results of this study. It was observed that there was a general increase in fasting blood glucose levels over the spectrum of CAD severity from normal patients to those diagnosed with the TVD. In a study conducted by Park et al in which the objective was to characterize the dose–response relationship between fasting glucose levels below those diagnostic of diabetes with cardiovascular events and when the levels rose above the normal value, the risk also gradually increased.7 The presence of T2D further augments these factors and can therefore induce adverse functional and structural changes to the vessel wall. It has been suggested that increased concentrations of free fatty acids may lead to the induction of inflammatory responses, worsen insulin resistance, and impair endothelium-dependent vasodilation.8
HbA1c levels have been able to identify individuals with prediabetes as having a worse cardiometabolic risk profile and more severe CAD as compared with those patients with normal glycemic levels.9 HbA1c levels have been known to be associated with an increased risk for vascular complications and have also been observed to be strongly correlated with CAD severity.10 The present study of this cohort of Trinidadian patients produced results that followed the same patterns as reported in the previous studies. High fasting blood glucose and increased HbA1c levels have been observed to be potential risk factors for cardiovascular events.11 Elevated glucose levels in the blood tend to change the structure and viscosity of the blood, causing it to potentially adhere to the sides of veins and arteries. This, therefore, causes blood vessels to become thicker and blood flow is then impaired. This process can then lead to atherosclerosis and other heart issues.12 These data were additionally supported by the strong positive correlation produced by HbA1c and CAD severity, suggesting that as these levels increase in the blood, so does the severity of CAD from normal to TVD. As stated by Dutta et al, with increasing levels of glycated hemoglobin, a significant increase was observed in the mean number of diseased vessels involved in CAD. They also reported a linear correlation between HbA1c and the number of vessels involved.10 The current study in the cohort of Trinidadian patients, therefore, added support to the results of the studies in the past.
Creatinine is a chemical waste product that is generated from muscle metabolism. Mild forms of creatinine elevation are also associated with poor cardiovascular outcomes. Korkmaz et al stated that patients in the highest creatinine group also had the highest total stenosis irrespective of their age and gender.13 Their study aimed to show whether creatinine has any influence on angiographically shown stenosis and extension of coronary atherosclerosis in patients with stable CAD.13 Another study found that small increases in the creatinine levels of patients with systolic dysfunction after myocardial infarction, over a specified period, were defined as worsening renal function. Creatinine was then characterized as a measure of renal function.14
Another group recently demonstrated that NT-proBNP is independently predictive of the severity of coronary disease diagnosed by coronary angiography. It was observed that the diagnostic value of NT-proBNP seemed to have increased with the severity of atherosclerotic lesions, especially those of TVD and left main artery disease. Levels of natriuretic peptides in the blood were detected to be increased across the CAD severity spectrum.15 The NT-proBNP patterns in our study patient population were found to be consistent with the above-mentioned literature. NT-proBNP levels were also seen to be correlated with the number of vessels involved in CAD, from no disease to TVD. NT-proBNP is the inactive fragment of its prohormone and is released by the cardiac atria and ventricles in response to elevated volume and filling pressures.16 This marker is released into the circulation in response to ventricular stretch and cardiac ischemia and has therefore emerged as a biochemical measurement of cardiac performance.15 Since this is a physiological hormone and is actively secreted under ischemic conditions, it serves as a marker for myocardial ischemia. Previous studies have shown that expression of the BNP gene is upregulated by myocardial hypoxia and this may be the probable mechanism.17 Thus, NT-proBNP has been characterized as a relevant emerging biomarker of CAD, and heart disease in general. It is predictive of CAD presence and severity, and this Trinidadian population of CAD patients seemed to follow a very similar pattern.
Blood concentrations of soluble ST2 are elevated in inflammatory and heart diseases, and this marker can be considered as a valuable prognostic variable in these conditions. Increases in soluble ST2 at baseline have been found to be associated with long-term all-cause and cardiovascular mortality in subjects having stable CAD.18 Soluble ST2 has also been observed to be a marker of myocardial fibrosis and remodeling.6 In addition to this, soluble ST2 has been explored to be able to predict mortality in heart failure patients and may also be able to identify heart failure patients at a higher risk of sudden cardiac death.6 This may be a possible explanation of why this parameter produced no significant pattern or correlation with the spectrum of CAD severity in our study. Our patients were not categorized based on the presence or absence of heart failure, stable or unstable CAD. Further study is therefore required in this area of these Trinidadian cardiac patients.
It has been suggested that natives of South Asians tend to have increased mortality rates with clinical appearance of CAD at early life due to their lifestyle and genetic susceptibility. Due to individuals of Indian descent having more traditional risk factors at earlier ages, this can explain the prevalence of premature CAD in this group. In addition, it has been found that the presence of abnormal lipid profile has a higher characteristic of CAD risk in South Asians when matched to other ethnic groups.19 Moreover, the association between alcohol consumption and cardiovascular mortality and morbidity has been debated for a long time. Several international comparisons show a negative association between alcohol usage and mortality due to coronary heart disease. Nevertheless, in the Regional Heart Study of 22 towns in Great Britain, a positive correlation was observed between the population of heavy drinkers in a town and mortality from coronary heart disease.20 Our observation of CAD status with respect to alcohol consumption in this study was in line with the previous reports that found no significant association between the two. Changes in various ethnic groups may be due to their risk factors and intensity of CAD. Various ethnic groups are subjected to develop CAD to an extent, causing a raise in frequency or intensity of disease in those populations. This trend has been shown in both developed and developing countries.21
For several decades, it has been believed that coronary heart disease is distinctly more common in men than in women. In both sexes, however, coronary heart disease increases with age.22 According to a study conducted by Hertzer et al, the overall occurrence of severe CAD is significant in all age groups; however, a higher incidence of severe CAD determined by coronary angiography was observed with each decade of advancing age and is also supported by the findings in this study.23 Another study has reinforced that women had a tendency to develop cardiovascular diseases 7 to 10 years later than men.24 Studies have explored the possible reasons why heart disease was more frequent in men. Gender differences were discovered in psychosocial and behavioral coronary risk factors in men, including excessive alcohol consumption and smoking. The dealing ability of men with stressful situations seems to be less adaptive physiologically. This possibly increased their risk for coronary heart disease.25
Given the unselected nature of the patient selection, the authors could not control for the possibility of referral bias inflating the rates of males versus females in our patient population. The hospital at which the study was conducted performs cardiac catheterization procedures for the entire island's public health care system, and it is therefore reasonable to assume that the patient population is representative of the island's CAD population.
Conclusion
This study investigates whether the anthropometric, biochemical, and metabolic profiles of patients undergoing coronary angiography predict the presence and severity of CAD in a Trinidadian cohort. There is a paucity of data for the Caribbean as it pertains to noncommunicable diseases in general and cardiovascular disease specifically. The economic challenges of the region as a whole mean that earlier risk stratification of patients potentially at risk of severe CAD can mean more targeted utilization of costly resources with a potentially greater return on investment for developing countries.
A few parameters were well correlated and well associated with the severity of CAD after diagnosis by the process of coronary angiography. These biochemical parameters included FBS, NT-proBNP, creatinine, and particularly, glycated hemoglobin. The clinical parameters observed to be well associated with CAD severity in this population were presence of T2D, ethnicity (Indo-Trinidadian), and age. One variable which was expected to produce similar results to that of NT-proBNP and HbA1c was soluble ST2. However, this marker showed no statistically significant correlations with CAD severity. Further study with this population will therefore need to be conducted. Overall, FBS, glycated hemoglobin, NT-proBNP, and creatinine could be used as a panel of potential prognostic biomarkers of CAD severity. Our study will provide the basis for longer term studies on larger Caribbean patient populations with perhaps more diverse ethnic groups. This will provide more insights on these key biomarkers that predispose to CAD.
Conflict of Interest
None declared.
Funding
The authors would like to thank Campus Research and Publication fund, The University of the West Indies for providing the grant to conduct this study.
References
- Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442.
- [CrossRef] [PubMed] [Google Scholar]
- Economic burden of cardiovascular diseases in the enlarged European Union. Eur Heart J. 2006;27(13):1610-1619.
- [CrossRef] [PubMed] [Google Scholar]
- Ministry of Health- Trinidad and Tobago 2013 Accessed April 5, 2018, at: https://www.health.gov.tt/news/newsitem.aspx?id=417
- Clinical profile of patients undergoing coronary angiography with special reference to complications of coronary angiography. Int J Advance Med. 2017;4(04):1170-1174.
- [CrossRef] [Google Scholar]
- Coronary Angiogram Diagnosing Heart Disease [Internet] MedicineNet Accessed August 9, 2018, at: https://www.medicinenet.com/coronary_angiogram/article.htm#what_is_a_coronary_angiogram
- [Google Scholar]
- Combined use of high-sensitivity ST2 and NTproBNP to improve the prediction of death in heart failure. Eur J Heart Fail. 2012;14(01):32-38.
- [CrossRef] [PubMed] [Google Scholar]
- Fasting glucose level and the risk of incident atherosclerotic cardiovascular diseases. Diabetes Care. 2013;36(07):1988-1993.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular disease in type 2 diabetes from population to man to mechanisms: the Kelly West Award Lecture 2008. Diabetes Care. 2010;33(02):442-449.
- [CrossRef] [PubMed] [Google Scholar]
- Individuals with prediabetes identified by HbA1c undergoing coronary angiography have worse cardiometabolic profile than those identified by fasting glucose. Diabetol Metab Syndr. 2014;6(01):138.
- [CrossRef] [PubMed] [Google Scholar]
- Glycated hemoglobin (HBA1C) correlation with severity of coronary artery disease in non-diabetic patients - a hospital based study from North-Eastern India. J Clin Diagn Res. 2016;10(09):OC20-OC23.
- [CrossRef] [PubMed] [Google Scholar]
- Severity of renal vascular disease predicts mortality in patients undergoing coronary angiography. Kidney Int. 2001;60(04):1490-1497.
- [CrossRef] [PubMed] [Google Scholar]
- The Connection Between Diabetes, Heart Disease, And Stroke [Internet] TheDiabetesCouncil.com Accessed July 3, 2018, at: https://www.thediabetescouncil.com/the-connection-between-diabetes-heart-disease-and-stroke/
- [Google Scholar]
- Serum creatinine is independently associated with angiographic extent of coronary artery disease in patients with stable angina pectoris. Anadolu Kardiyol Derg. 2011;11(05):407-413.
- [CrossRef] [Google Scholar]
- Increase in creatinine and cardiovascular risk in patients with systolic dysfunction after myocardial infarction. J Am Soc Nephrol. 2006;17(10):2886-2891.
- [CrossRef] [PubMed] [Google Scholar]
- Is N-terminal pro B-type natriuretic peptide (NT-proBNP) a useful screening test for angiographic findings in patients with stable coronary disease? Am Heart J. 2006;151(03):712.e1-712.e7.
- [CrossRef] [PubMed] [Google Scholar]
- Can we predict the severity of coronary artery disease in patients with stable angina using NT-ProBNP? Anadolu Kardiyol Derg. 2006;6(03):235-238.
- [Google Scholar]
- Increased cardiac BNP expression associated with myocardial ischemia. FASEB J. 2003;17(09):1105-1107.
- [CrossRef] [PubMed] [Google Scholar]
- Increased soluble ST2 predicts long-term mortality in patients with stable coronary artery disease: results from the Ludwigshafen risk and cardiovascular health study. Clin Chem. 2014;60(03):530-540.
- [CrossRef] [PubMed] [Google Scholar]
- Coronary artery disease in South Asians. Cardiol Rev. 2012;20(06):304-311.
- [CrossRef] [PubMed] [Google Scholar]
- Alcohol and coronary heart disease. Int J Epidemiol. 2001;30(04):724-729.
- [CrossRef] [PubMed] [Google Scholar]
- Ethnic differences in the risk factors and severity of coronary artery disease: a patient-based study in Iran. J Racial Ethn Health Disparities. 2018;5(03):623-631.
- [CrossRef] [PubMed] [Google Scholar]
- Sex, age, cardiovascular risk factors, and coronary heart disease: a prospective follow-up study of 14 786 middle-aged men and women in Finland. Circulation. 1999;99(09):1165-1172.
- [CrossRef] [PubMed] [Google Scholar]
- Coronary artery disease in peripheral vascular patients. A classification of 1000 coronary angiograms and results of surgical management. Ann Surg. 1984;199(02):223-233.
- [CrossRef] [PubMed] [Google Scholar]
- Gender differences in coronary heart disease. Neth Heart J. 2010;18(12):598-602.
- [CrossRef] [PubMed] [Google Scholar]
- Why do men get more heart disease than women? An international perspective. J Am Coll Health. 2000;48(06):291-294.
- [CrossRef] [PubMed] [Google Scholar]



