
Translate this page into:
Innovations in Strengthening Medical Education in India
DR. K.L. WIG ORATION delivered during NAMSCON 2015 at the All-India Institute of Medical Sciences, Patna.
Correspondence : Dr. Rajoo Singh Chhina, Office of Dean Academics, Dayanand Medical College and Hospital, Tagore Nagar, Civil Lines, Ludhiana-141001, E-mail: drrajoosingh@ gmail.com.
Abstract
There is a disconnect between the objectives of medical education in the country and the actual training being imparted. The present system of discipline based MBBS Curriculum has many inherent disadvantages eg. Compartmentalized teaching, poor development of problem solving skills, failure to generate interest in students and acquisition of dissociated knowledge are few of them. The SPICES model of medical education ie. (Student centered, Problem based, Integrated, Community oriented, Elective enabling and Systematic exposure) may be better suited to our country. Assessment system and examination system need a very drastic change based on the needs of the Community and the stakeholders in the healthcare section. Internship programme needs to be totally revamped. The acquisition of practical skills using newer medical education technology like DOPS (Directly Observed Practical Skills), one minute preceptor and other newer methods needs to be incorporated. In our study on “DOPS” interns we found the usefulness of this methodology (FAIMER study - Chhina RS).The use of technology has revolutionized the world eg. in Space technology, Computer Sciences, Social marketing Strategies. There is an urgent need to incorporate the “MOOC” model and the Social media eg. Facebook, Twitter, We chat, Whatsapp for better coverage and more useful teaching modules. In our study, we found “Facebook” teaching to be an important component of improving the teaching methodology and acquisition of knowledge by students (FAIMER study- Sharma Anu & Chhina RS). The “Feedback” technique for improvement in the needs of student knowledge base, their aspirations, what they thought is appropriate in teaching skills and methodology was studied and powerful conclusions have been drawn in our institution. (FAIMER study-Singh Daljit). The postgraduate training seats needs to be modified as the disease burden load in the country requires. A study done by us showed a total disconnect between the need and the available resources in the State of Punjab. The requirements of the Community, Medical students, Healthcare providers and patients need to be advanced in an objectively scientific, need oriented manner in relation to medical education in India.
Keywords
Medical Education
DOPS (Directly Observed Procedural Skills)
MOOC (Massive Open Online Course)
FAIMER (Fellowship, Foundation for Advancement of International Medical Education & Research)

Innovation is a noun that means something new. Lot of debate is ongoing on the issue of the Medical Education in India. The State of Medical Education in India presents a scenario marked by rhetoric and wishful thinking rather than concrete steps in right direction. The search for a need based curriculum is not new. It has been felt for ages, but the curriculum has not really changed. It is an oft-repeated criticism that our medical colleges are producing graduates who are not well equipped to tackle the health care needs of the society (1).
The Medical Council of India (MCI) has recommended both horizontal (eg. Anatomy, Physiology, Biochemistry) and vertical integration (e.g. Anatomy with Surgery) to be introduced throughout the curriculum. The latest MCI guidelines stipulate that undergraduate medical education should be oriented towards health and community. Students training must aim at inculcating scientific temper, logical and scientific reasoning, clarity of expression, and ability to gather and analyze information (2).
The students in today's era of evidence based medicine favor “hard” clinical knowledge over “soft” health promotion/disease prevention, knowledge and skills. This has also been commented upon and discussed in the international forum like World Health Organization South East Asia Regional Organization (WHO SEARO) Health Minister's Meeting (3).
Learning Approach :
Students learn with the following three approaches commonly followed:
Superficial Learning
Deep Learning
Strategic Learning
Superficial learning is based on the approach of 'Recall' and the students without understanding of the facts memorize and this forms the base of Miller's Triangle knows and is the lowest level of learning.
Deep Learning is based on understanding of the facts and figures and also needs a comprehensive and critical review and understanding of the subject. Deep Learning is needed for life long understanding and learning process that forms the basis of clinical practice in future. The “Knows How” of the Miller's triangle is based on this approach (Fig.1) (4).
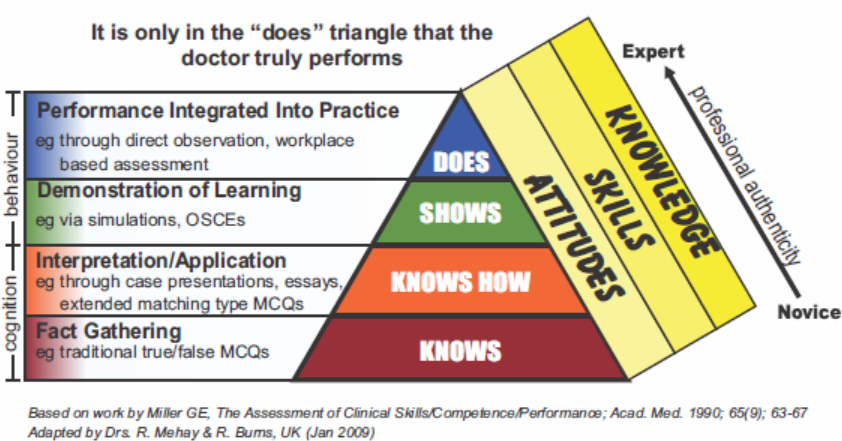
- Miller’s Prism of Clinical Competence (aka Miller’s Pyramid)
Students are likely to adopt a deeper approach to their learning and achieve quality learning outcomes. When teachers provide for:
Motivation and curiosity
Student independence
Student choice
Opportunities to work with other people
Low threat environment
Challenging environment
Frequent, constructive and supportive feedback
An emphasis on higher levels of objectives.
The strategic learning approach inculcates a plan with the problem based learning. What is needed how much is needed and how it will help the top of the Miller's triangle 'Does' becomes an integral part of the learning experience.
The learning/teaching triangle shown below shows the learning percentage for different models of teaching (Learning Pyramid) (Fig.2).
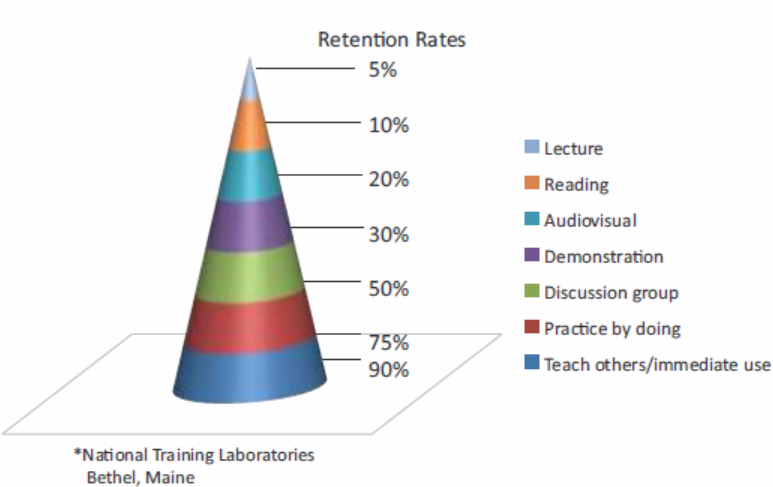
- The Learning Pyramid*
From above it is clear that typical classroom teaching is inadequate for proper retention rates and modalities of teaching fare better (5).
Current medical education should prepare healthcare professional to be able to deal with the intricacies of healthcare system in addition to their clinical skills, economic knowledge and national healthcare needs have to be incorporated into the medical curriculum. This change is needed at all levels and the sooner it is done, the better it is for the dynamics of medical education.
Edu-tainment :
Education and entertainment have to be combined and the rhetoric of medical education being boring, a repetitive and non-competency based is being debated for a long time. Medical Education has a history of tinkering with the medical curriculum without realizing larger educational objectives. Medical colleges have to create a true learner centered environment that makes active, self directed learning under the facilitation of interested faculty members a possibility. When Education and Entertainment are combined the word “Edu-tainment” emerges and true learning/life long learning occurs in the non-threatening, conducive, flexible and relaxed environment.
Innovations in Medical Education :
Innovations tried and validated by us have been in the following areas:
Teaching
Curriculum
Assessment
Use of technology
Teaching methodology is variable from regions, countries and person. Student centered teaching is the buzz words and following points are worthy of mention:
Students are active in planning, rehearsing and assessing outcomes.
Students make the choices on what and how to learn.
Learning across the curriculum, flexible and can occur anywhere.
Teacher is more of a mentor, guide and a facilitator.
Emphasis is on a long time/ life long learning.
The acronym SPICES refers to six main concepts in Medical Education- student centered teaching, problem based learning, an integrated curriculum, and community based teaching, electives with a core and the use of systematic method. An awareness of these principles means the medical students can take a more active role in their learning. Students who are well informed about medical education principles, such as the SPICES criteria, are more likely to be able to provide constructive feedback about their own medical education experience, contributing in the long term to course (6).
Technology and Medical Eduaction :
Use of technology has revolutionized the medical education in it's various formats. Journal of Graduate Medical Education, June 2014 has article on the use of smartphones in “Graduate Medical Education” (GME). There are many ways that mobile phones applications (apps) can be used for medical education and bedside case to complement traditional in class teaching methods. Although the initial impulse of some educators might be that the smartphones, ipads and computer might be a distraction, but the myriad uses prompt us to consider the paradigm shift.
In “Smartphones, Trainees and Mobile Education: Implications for Graduate Medical Education,” Short et al review the many ways that mobile phone applications (apps) can be used for education and bedside care to compliment traditional in classroom teaching approaches. Are we talking full advantage of teaching through mobile platforms? We propose that the “teachable moment” has expanded. iPads preloaded with digital resources, including textbooks and podcasts of lectures; the ipads also have the ability to interface with digital stethoscopes, portable ultrasound technology and encrypted electronic health records.
The following questions may be considered by the GME community:
What are the most effective models of new technology?
Can targeted learning be individualized using new technology?
Are there metrics to determine the quality and validity of open access, online content in medical education?
Can technologies be harnessed to assess competencies and milestones?
How do we use technology to facilitate p atient centered care (eg. Communication, patient education, shared decision making)?
How can the electronic health record serve as learning tool for residents?
What are the standards of professionalism and how does one teach them to learners in this new age of open, collaborative social media?
Can we establish standards for sharing patient information via technology and social media?
From the perspective of a “digital educator", how can we demonstrate scholarship for faculty.
The concept of 'MOOC' needs to be emphasized (7).
Inspiring innovations in medical education what is the bright idea? Using facebook as a medium of interface in students has yield good results in our centre (Sharma Anu et al.).
Feedback and Medical Education :
Feedback of students (Anurag Chaudhary et al.)
Appraisal of undergraduate feedback (Hemlata Badyal et al.)
Feedback of Teachers (Dr. Daljit Singh et al.)
We have conducted studies on the above three parameters and have reached a conclusion that a positive constructive feedback with scope of improving the outcomes remains the backbone for any system to progress. Anything which is assessed on a periodical basis is likely to show improvement over a period of time. The student/Faculty feedback improved our understanding of the complexity of student faculty interaction. When student feedback was appraised it showed a linear correlation with improved outcomes.
The Internship Year :
We have tried for the competency based medical education in interns. Internship is a phase of training when new graduate is expected to aquire skills under supervision, so that he/she may become capable of functioning independently. Often new graduates go through this period without a clear aim. We conducted an orientation programme before fresh graduates started their 1-year internship to familiarize them with their clinical tasks and their role in the community (8).
The internship is a very important part of educational training of Medical Student but it has deteriorated over time and it has reduced it's relevance and value to the students. The internship currently “UNASSESSED” does not serve the purpose of giving hands on experience because the intern's focus and target is the postgraduate examinations rather than acquiring the clinical skills.
Changes and innovation which have been tried:
Period must be assessed.
Time should be spent on acquiring and enhancing skills.
Skill development must ensure competence in delivering life saving measures.
The use of log books/ procedure books has been tried in our institution.
Structuring of training programme of interns in the department of medicine and assessment of procedural skills using “Directly observed procedural skills” (DOPS) was used and the following conclusion were made that the use structured protocol for skill assessment by DOPS is helpful methodology for improvement of knowledge and procedural skills of interns.
CME in Undergraduates :
CME in Medical Education has been shown by us to be of value in the pre and post CME assessment of the knowledge and understanding of the subject by the students.
Thesis Writing :
Thesis writing as a protocol is being followed in the Country. It needs to optimized and in line with the Health Care needs of the society.
The downhill course in some aspects needs to be reversed. The prospects of medical education have a positive outcome provided, we do the needed changes at the earliest.
REFERENCES :
- International Handbook of Medical Education. In: Westport, Connecticut. London: Greenwoof Press; 1994. p. :207-230.
- [Google Scholar]
- Innovations in Teaching/Learning Methods for Medical Students: Research with Mentoring. Indian J Public Health. 2013;57:144-146.
- [CrossRef] [PubMed] [Google Scholar]
- The assessment of clinical skills/ Competence/ Performance. Acad Med. 1990;65(9):63-67.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with medical knowledge acquisition during Internal Medicine Residency. J Gen Intern Med. 2007;22(7):962-968.
- [CrossRef] [PubMed] [Google Scholar]
- Technology in Adequate Medical Education shifting the Paradigm and Advancing the field. J Grad MedEdu. 2014;6(2):195-196.
- [CrossRef] [PubMed] [Google Scholar]
- Structured Internship Orientation Programme for Undergraduate Students: Easy Transition to Clinical Work. Natl Med J India. 2010;23:160-161.
- [Google Scholar]



