
Translate this page into:
Spatial Epidemiology of COPD in Delhi, India
Address for correspondence Arun Kumar Sharma, MD, National Institute for Implementation Research on Non-Communicable Diseases, Jodhpur 342005, Rajasthan, India (e-mail: a.sharma@icmr.gov.in).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) and bronchial asthma are the most common chronic respiratory illnesses. COPD is one of the three most common causes of death worldwide. The main burden of mortality from COPD is seen in Latin America, sub-Saharan Africa, India, China, and South-East Asia. Absence of true prevalence values and mortality burden hinder planning and operationalization of public health interventions for prevention, control, and treatment of the disease. Further, the aggregated value of prevalence estimates calculated for a whole city or a larger geographical area does not provide the location of patients and presence of locally prevalent risk factors. The objective of this study was to understand the spatial distribution of COPD in a large, highly polluted city of a developing country.
Materials and Methods
A cross-sectional community-based study was conducted in the National Capital Territory of Delhi (NCTD). All surveyed households were geocoded. GOLD screening criteria and pulmonary function tests using portable digital spirometer were used for diagnosis of COPD.
Results
Results are presented as a series of maps depicting spatial epidemiology. Overall prevalence rate was 9.8/1,000 population. Highest prevalence was seen in industrial area. Most of the spatial hotspots were seen in industrial and slum areas. Similarly, Kernel density was also highest in industrial area.
Conclusion
In the city of NCTD, we found the COPD being distributed in all types of habitations but spatial distribution helped us understand clustering of cases and compare prevalence rates in subunits of residential clusters within a metropolitan city.
Keywords
COPD
spatial distribution
spatial hotspots

Introduction
Chronic obstructive pulmonary disease (COPD) and bronchial asthma are the most common chronic respiratory illnesses. COPD is one of the three most common causes of death worldwide.1 The Global Burden of Disease (GBD) Study estimated that in 2015 COPD affected 104.7 million men and 69.7 million women globally, and that between 1990 and 2015 the prevalence of COPD increased by 44.2%.2 Globally, in 2017, the five leading causes of disability-adjusted life years lost were neonatal disorders, ischemic heart disease, stroke, lower respiratory infections, and COPD.3 The main burden of mortality from COPD is seen in Latin America, sub-Saharan Africa, India, China, and South-East Asia.4 Deaths from COPD are predicted to rise to 4.4 million per year in 2040 and by then, COPD is predicted to be the fourth most important cause of years of life lost.5
The GBD estimates that the number of COPD cases in India has already increased from 28.1 million in 1990 to 55.3 million in 2016, an increase in prevalence from 3.3% to 4.2%.6 Unfortunately, there has been no nation-wide study conducted to assess the burden of COPD and the estimates are based on studies conducted in different parts of the country, at different points in time and using different methodologies, that made home opine that the lack of robust real-time nation-wide data does plague India as well; however, multiple studies from 1994 to 2010 show increasing trends of COPD morbidity and mortality.7
The morbidity and mortality burden of a disease can be truly estimated if the prevalence can be determined through community-based studies and all mortalities are recorded and reported in a timely manner. Absence of true prevalence values and mortality burden hinder planning and operationalization of public health interventions for prevention, control and treatment of the disease. In absence of availability of such data, estimates of the burden of disease are projected based on hospital-based studies or studies conducted on small sets of populations. Such estimates have the probability of being erroneous in terms of underestimation or overestimation of the burden. The other source of error is changes in the disease magnitude over a period of time due to temporal variations in the disease burden, thereby necessitating the need for repeated surveys at regular intervals. Further, the aggregated value of prevalence estimates calculated for a whole city or district or a larger geographical area does not provide the location of patients and we are not able to understand if there are any locally prevalent factors that increase the risk of occurrence of COPD in that particular area. Environmental risk factors for COPD are also heterogeneously distributed across the habitations and thus their contribution to causation of COPD can be better estimated if we have access to such data at local level. To understand the local geographical distribution of the COPD cases and its risk factors, we conducted this study. The primary objective was to understand the spatial distribution of COPD and the impact of local environmental factors on distribution of the cases of COPD.
Materials and Methods
The study was conducted in National Capital Territory of Delhi (NCTD) in India. Delhi is spread across 1,484 km2. It is located in the coordinates of 76.84°E, 28.41°N, by 77.35°E, 28.88°N. In the larger geographic context, Delhi is situated between the Himalayas and the Aravalli Mountain ranges in the north and south, respectively, and the River Yamuna flows through the eastern part of the city. According to the 2011 census, Delhi's city proper population was over 11 million, the second-highest in India after Mumbai, while the whole NCTD's population was ∼16.8 million (see http://unccdcop14india.gov.in/about-delhi). NCTD is divided into 11 administrative districts. The inhabitations are distributed in purely residential, residential-cum commercial, and designated industrial areas of the city. Besides, there are unauthorized slum clusters spread throughout the city. Hence, there are pockets of inhabitations, where people are exposed to industrial pollutants or to the pollution caused by vehicular exhaust and biomass fuel burning in commercial areas. There are designated villages in the city. From the socioeconomic perspectives, housing facilities are classified as high-, (HIG) middle-, (MIG) and low-income group (LIG)housing, rehabilitation colonies (a replacement residents of slums), slums, and villages. To capture different types of physical environments, it was ensured that the survey includes all types of residential areas and all categories of housing. In all, 11 colonies were selected using purposive sampling method.
Sample Size
In a study conducted in Ludhiana, India, total 17, 637 adult persons were screened and the prevalence of COPD was found to be 3.5/1,000 population.8 Using this prevalence value, assuming a relative precision of 20%, at 95% level of confidence, the required sample size is 27 343 adult persons. So, it was proposed to screen 28,000 adult persons for the determination of prevalence of COPD. In urban areas, 66.6% of the population belong to 15 to 59 years age group (Census 2011). Using this data, to get 28,000 in 18 to 60 age group, ∼37,240 total population were to be screened. Given an average household size of 4.61 in urban India, the total number of households to be screened were 8,078. The study was expected to detect 98 COPD cases.
Sampling
Sampling units were residential colonies in the NCT of Delhi. Following colonies were selected as per convenience yet representing the land use pattern and varied ambient air pollution. Location of colonies is depicted in ►Fig. 1. All households were contacted in each colony. The geocoordinates of each housing unit were recorded using global positioning system device, Juno SA Handheld, manufactured by Trimble Navigation Limited, Westminster, Colorado, United States.

- Distribution of surveyed colonies and households.
Data Collection
A close-ended questionnaire was developed in Hindi and pretested prior to starting data collection. Part I was used for obtaining demographic details of the household and also for empirical assessment of air quality in the household. Air quality was assessed by cross-ventilation, physical presence of dust, disposal of solid and organic waste, presence of insects, and type of fuel used for cooking.
Part II of the questionnaire was used for recording details about any suspected/confirmed case of COPD in the family. It included personal profile of the patient, duration of stay in the city, and type of accommodation used for living. Empirical assessment of potential exposure to risk factors for COPD was performed by asking questions regarding current and past jobs, modes of transportation used in commuting to workplace, nature of work, air quality at work place, and exposure to active and passive smoking. This questionnaire also included a modified version of GOLD screening criteria for COPD; it is a Likert scale-based questionnaire having 7 items and a 0 to 5 scoring for each item. Maximum total score possible was 35. A score of 10 or above was considered indicative of COPD.9 Validated Hindi version of the questionnaire was available for download and it was free for use. History regarding diagnosis, treatment, and presence of comorbidities like diabetes mellitus, hypertension, coronary artery diseases, chronic kidney diseases, and any mental illness was included in the part II of the questionnaire. Portable handheld digital spirometer was used for assessing the lung functions of the suspected and confirmed COPD patients. The UNI-EM PC Based Spiromin spirometer, manufactured by Universal Medical Instruments, Delhi, India, was used along with its Windows-based software for capturing lung function parameters.
The study was approved by the Institutional Ethics Committee (Human Research) of University College of Medical Sciences, Delhi. Informed written consent was obtained in approved form from the respondent in each surveyed household. A patient information sheet containing details of the study, associated risks, benefits and contact nos. of the principal investigator, and data collector was given to the participants.
In this article, we are presenting the spatial epidemiology of COPD in Delhi.
Results
The individual colonies and households in those colonies that were surveyed are shown in ►Fig. 1 In all 11 residential colonies were selected covering different land use patterns. In all 8,510 households were contacted covering a population of 40,040. Fifty three percent of the population were male, and 46% were above 30 years of age. Out of 443 suspected cases, diagnosis of COPD was confirmed in 394 cases, based on spirometry and/or available prescriptions and hospital discharge reports. Overall prevalence rate was 9.8/1,000 population and among population over 30 years of age, prevalence rate was 21.2/1,000. The location of confirmed cases of COPD is shown in ►Fig. 2A. We calculated COPD prevalence rate according to the land use pattern classification as depicted in ►Fig. 2B. The highest prevalence rate was seen in the industrial area (13.2/1,000 population) and the MIG type housing in Dilshad Garden. The JJ colonies (slum settlements) had relatively less density of the disease, though absolute number of cases were more in the JJ colonies. The least prevalence rates were seen in the rural areas, both East and South Delhi as well as in the low-income housing in North Delhi (Jahangirpuri). In fact, the rates in industrial and MIG colonies were double the rates of rural areas. We also calculated the prevalence rates in population of age 30 years and above as shown in ►Fig. 2C.

- (A) Aggregated location of chronic obstructive pulmonary disease (COPD) cases. (B) COPD prevalence rates in total population. (C) COPD prevalence rates in population above 30 years.
We performed a cluster and outlier analysis for COPD cases as shown in ►Fig. 3A. Practically, there was no significant clustering effect seen in any part of the city but low-high outlier clustering was seen in the rural area of South Delhi and LIG housing in North Delhi. But we did identify COPD hotspots. Within colonies also there was clustering of cases creating a few hotspots, but predictably the maximum hotspots were seen in industrial area, a part of the Jahangirpuri Colony and also in the Mansarovar Park area of East Delhi, as shown in ►Fig. 3B. Using nearest neighbor approach, hotspots were seen in several areas including the industrial area, the LIG housing, and unexpectedly in the village in South Delhi. We also explored the optimized Hot Spot Analysis tool using Getis-Ord GI* statistic. This method uses optimization of available number of observation points (in our analysis, each COPD patient is an observation point). Our data fulfilled the criteria of minimum 30 observations in a polygon; hence, the analysis was statistically valid. But by this method, the hotspots were found to be in Dilshad Garden only (►Fig. 3C).
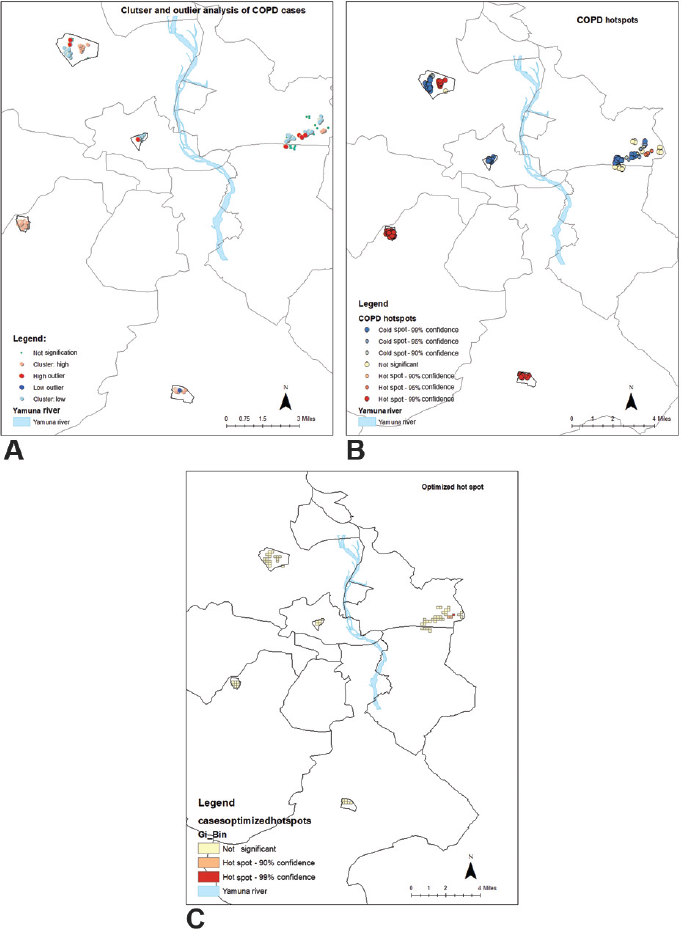
- (A) Cluster and outlier analysis of chronic obstructive pulmonary disease (COPD) cases. (B) Hotspots of COPD in National Capital Territory of Delhi (NCTD). (C) Optimized hotspots of COPD in NCTD.
If we look at the COPD Kernel density map, maximum density was seen in East Delhi that could have been probably due to the fact that maximum surveyed population was in East Delhi (►Fig. 4A).

- (A) Kernel density estimation of chronic obstructive pulmonary disease. (B) Ripley's K function graph.
Discussion
The spatial epidemiological exercise was performed to examine the spatial distribution of COPD cases. The absolute number of cases was highest in MIG and HIG colonies, but the prevalence rates were highest in the industrial area followed by the JJ colony. This finding is similar to the findings in Ludhiana, where the prevalence was also higher in industrial area compared with the other residential areas of the city.8 In Ludhiana, the overall prevalence rate was 3.17/1,000 population and in industrial area it was 4.2/1,000 population. This was much lower than the prevalence rate in NCT of Delhi that is 9.8/1,000 overall and 13.5/1,000 in industrial area. Thus, it may be inferred that other than industrial environment, air pollution may also be contributing significantly to higher prevalence in Delhi. However, in a few pockets of the industrial area of Ludhiana, where the living conditions were far more inferior, the prevalence rates were as high as 9.4/1,000 that was similar to the overall prevalence rates in Delhi. However, the overall population surveyed in Ludhiana was much smaller than that in Delhi.
We also compared prevalence rates among different land use patterns across the city. industrial area and MIG colonies showed highest prevalence rates. By changing the denominator from total population to population above 30 years of age, there was no change in the higher prevalence areas, namely industrial area and JJ colonies but the prevalence pattern changed in the JJ colony and LIG housing areas, thereby suggesting that the exposure and disease outcome varied with respect to age of the population. The older population in low socioeconomic housing areas was more likely to have been exposed to adverse environment, thus increasing COPD prevalence among them. This difference gets highlighted in spatial analysis.
We had hypothesized that there would be clustering of cases and it did happen, verified by hotspot analysis as well as by clustering analysis. However, there were no hotspots with respect to prevalence rates. To detect clustering, we used Ripley's K function. Ripley's K function looks at spatial clustering or dispersion of features at a series of distances or spatial scales. In the K function graph, the blue line represents the expected pattern, if the COPD cases were randomly distributed in the study area, whereas the red line represents the observed spatial pattern for the COPD cases' distribution (►Fig. 4B). As the distance increases from 800 to 1,400 m, there is a linear increase in clustering, but plateaus out after 2,800 m. This explains that clustering is restricted to colonies as predictably the colonies are spread out mostly between 800 and 16,00 m distance. Larger colonies like Jahangirpuri and Dilshad Garden are more widespread; hence, the slope continues to rise up to 2,800 m.
Conclusion
In the city of Delhi, we found the COPD is being distributed in all types of habitations but spatial distribution helped us understand clustering of cases and compare prevalence rates in subunits of residential clusters within a metropolitan city. This may be used for planning interventions related to prevention of occurrence of COPD as well as in providing access to healthcare to the COPD patients. Longitudinal studies in future will help us understand the temporal trends in distribution of COPD cases.
Conflict of Interest
None declared.
Funding
This study was funded by the HRD-Scheme of the Department of Health Research for Start-Up grant, Ministry of Health & Family Welfare, Government of India.
References
- Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095-2128.
- [Google Scholar]
- Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(09):691-706.
- [Google Scholar]
- Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859-1922.
- [Google Scholar]
- The GOLD Summit on chronic obstructive pulmonary disease in low- and middle-income countries. Int J Tuberc Lung Dis. 2019;23(11):1131-1141.
- [CrossRef] [PubMed] [Google Scholar]
- Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392(10159):2052-2090.
- [Google Scholar]
- The burden of chronic respiratory diseases and their heterogeneity across the states of India: the Global Burden of Disease Study 1990-2016. Lancet Glob Health. 2018;6(12):e1363-e1374.
- [Google Scholar]
- Pilot study of chronic obstructive pulmonary disease in an industrial town in India. J Health Pollut. 2019;9(21):190304.
- [CrossRef] [PubMed] [Google Scholar]
- Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(03):648-654.
- [CrossRef] [PubMed] [Google Scholar]



