
Translate this page into:
Assessment, localization of hearing loss and rehabilitation in children with cerebral palsy

*Corresponding author: Dr. Ekta Narang, MS(ENT), Department of ENT, Chacha Nehru Bal Chikitsalya, Geeta Colony, New Delhi, 110031, India. ektachhabra@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Mathur NN, Narang E. Assessment, localization of hearing loss and rehabilitation in children with cerebral palsy. Ann Natl Acad Med Sci (India) 2025;61:16-20. doi: 10.25259/ANAMS_5_2024
Abstract
Objective
This study was designed to assess hearing loss in children with cerebral palsy (CP) using brainstem evoked response audiometry (BERA), otoacoustic emissions (OAE), pure-tone audiometry (PTA), and impedance audiometry. The prevalence of hearing loss was studied in this group and the location of lesion causing hearing loss was found using the above tests. We also compared the efficacy of OAE and BERA as screening modality for the detection of hearing impairment in such children.
Material and Methods
The study was conducted on 100 patients (200 ears) with CP in the age group of 1–18 years. The patients were selected randomly from those presenting to the Outpatient Department (OPD) with a diagnosis of CP in Kalawati Saran Children’s Hospital. Investigations like BERA, transient evoked OAE (TEOAE), distortion product OAE (DPOAE), PTA, and impedance audiometry were done on them.
Results
On BERA, 58.5% children passed as per our criteria, and 41.5% failed the test. In all, 78% cases showed abnormal morphology of wave V. More than 50% of those who passed on BERA had poor morphology of wave V. Latency of wave V at 80 dB was prolonged in most cases. The mean latency of wave V was 6.159 msec. About 83.5% children failed on OAE testing according to our criteria, while only 16.5% passed.
Conclusion
The prevalence of hearing loss was calculated to be 41.5%. In most cases, the site of the lesion was found to be cochlea, as OAE was absent in most cases (83.5% of patients tested). OAE was found to be a less efficacious test as compared to BERA in detecting hearing loss.
Keywords
BERA
Cerebral palsy
Hearing
OAE

INTRODUCTION
Cerebral palsy (CP) is defined as “a group of permanent disorders of the development of movement and posture, causing activity limitation, that is attributed to non progressive disturbances that occurred in the developing fetal or infant brain.”1 The incidence of CP in the general population varies throughout the world at a rate of 0.1%–0.2% of live births in developed countries and is slightly higher in developing countries, with the risk of CP increasing with decreasing gestational age.2,3
CP is commonly associated with a spectrum of developmental disabilities. Besides motor abnormalities, a child with CP suffers from multiple handicaps like mental retardation, epilepsy, visual, hearing, speech, cognitive, and behavioral abnormalities.4 There are few published studies on the prevalence of hearing loss in CP. The incidence of hearing loss was reported to be between 7% and 37.5%, with the majority of studies commenting only on sensorineural hearing loss (SNHL).5–9 Lesions causing hearing loss potentially involve the organ of Corti, especially at the outer hair cells and the cochlear nerve.
Hearing loss, which is so commonly associated with CP, requires an audiological assessment for a definitive diagnosis.10 Such children who are not responsive can be tested for hearing loss using an auditory evoked potential that measures the lowest possible sound level, which produces a brain wave in the child.
Although SNHL in patients with CP has been known for more than 50 years, yet the site of lesion in these cases remains in controversy. Also, the assessment of hearing in CP patients has always been a difficult task. Both parents and treating physicians remain uncertain about the cause of deranged/no response to any auditory stimulus in these patients. Even in those cases where hearing loss is established, the location of lesion causing hearing loss remains uncertain. It is however possible with the spectrum of investigative means available with us now in the form of distortion product otoacoustic emissions (DPOAE), transient evoked otoacoustic emissions (TEOAE), brainstem evoked response audiometry (BERA), pure-tone audiometry (PTA), impedance audiometry, cortical evoked response audiometry (CERA), and functional magnetic resonance imaging(fMRI) to identify and evaluate the hearing loss and make an endeavor to locate the site of lesion in such cases.
Our patients were investigated by BERA, TEOAE, DPOAE. PTA and impedance audiometry were done in a few cases. BERA is an objective test to evaluate hearing threshold and to diagnose retrocochlear pathologies tests of the cochlear status, specifically outer hair cells.
MATERIAL AND METHODS
Subjects
This study was performed on 100 patients (200 ears) with CP in the age group of 1–18 years. The patients were selected randomly from those presenting to the Outpatient Department (OPD) in Kalawati Saran Children’s Hospital with a diagnosis of CP. The study was conducted from October 2005 to February 2007 by conducting BERA, TEOAE, DPOAE, PTA, and impedance audiometry on these patients. The procedure of these hearing tests was explained to the parents and an informed consent was taken for conducting these tests. The tests were carried out in a double-wall sound treated room within permissible noise limits. Patients were followed up thereafter to the extent possible for the hearing rehabilitation.
Methods
BERA was done using Hortmann Neurootometrie BERA Soft @ 1995 by Hortmann Gmbh. Three surface electrodes were applied—one over each mastoid and the third over the forehead. Stimuli were given in the form of clicks which were broadband, in rarefaction phase, with an intensity of 60 dB (decibels). Around 2000 such clicks at the rate of 30/sec were given to the ear being tested. The contralateral ear was suitably masked by white noise. Waves I, III, and V (Jewett and Williston’s nomenclature) were looked at for the absolute latency, interpeak latency, and morphology. The passing criteria used for BERA was the presence of wave V at 60 dB HL (hearing loss). A similar procedure was repeated on the other ear of the same child.
TEOAE recordings were obtained using Hortmann Neurootometrie-Octavus (Germany) @ 1994; V5ILO OAE 88 Dpi Otodynamics Limited System. TEOAE probes fitted with disposable soft tips were used for recording TEOAE. Tips of various sizes were used depending on the size of the child’s external auditory canal. A snug fit of the probe was ensured. A set of four clicks were given as stimulus. The first three clicks were given for a duration of 80 msec at 80 dB SPL (sound pressure level). The fourth click was of opposite polarity and of three times the amplitude as compared to the first three.
The passing criteria of TEOAE were: (a) The response was reproducible 50% of times the test was performed; and (b) Any of the three frequencies tested (1.0,1.5,2.0,3.0,4.0 kHz) had 3 dB more power in the response spectrum than the noise spectrum.
DPOAE was done using Hortmann Neurootometric-Octa (Germany) 1994; V5 ILO OAE 88 Dpi Otodynamics Limited System. DPOAEs were recorded for both ears using the sweep stimuli ranging from 500 Hz to 8 kHz. L1 and L2 were set at 65 dB. The three points per octave were adopted for examination. Best probe fit was ensured to reduce the noise floor effects. In this study, DPOAE was taken to be present when its amplitude was 3 dB or more above the noise floor level.
Impedance audiometry was done by Impedance Audiometer AT235 Interacoustics A/S; Assens, DC-5610 Assens (Denmark). The type of tympanogram was noted. Tone above 80 dB were presented to the test ear and reflex picked up with a probe. The presence or absence of reflex was noted.
PTA could be done in only a few patients using an advanced Digital Audiometer AD-200 (ALPS) in similar settings. The diaphragm of the headphone was placed over the opening of the external auditory meatus. The hearing thresholds for frequencies of 250, 500, 1000, 2000 Hz were noted.
RESULTS
The distribution of neuromotor disturbance was studied. A maximum number of children (54%) with CP had quadriplegia, 21% hemiplegia, and 19% suffered diplegia. Spasticity was the most common type of neuromotor disturbance found in 91% of the children in this study group.
While 58.5% children passed on BERA according to our criteria, 41.5% failed the test [Figure 1]. The passing criteria used for BERA was the presence of wave V at 60 dB HL; 78% cases showed abnormal morphology of wave V. More than 50% cases that passed in BERA had poor morphology of wave V. Latency of wave V at 80 dB was prolonged in most cases [Table 1]. The mean latency of wave V was 6.159 msec [Table 2].
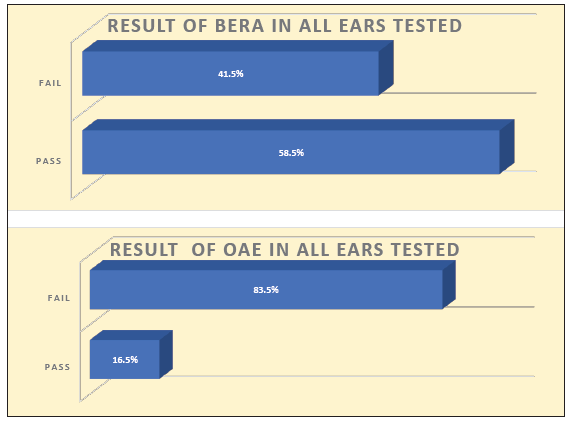
- Result of BERA and OAE in all ears tested. BERA: Brainstem evoked response audiometry, OAE: Otoacoustic emissions.
| Wave morphology | Frequency | Percent |
|---|---|---|
| Normal | 44 | 22 |
| Abnormal | 156 | 78 |
| Total | 200 | 100 |
| Ear tested | Number | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|---|
| Right side | 86 | 4.3 | 7.8 | 6.101 | 0.5608 |
| Left side | 88 | 5.1 | 7.6 | 6.216 | 0.5675 |
SD: Standard deviation
On otoacoustic emissions (OAE), 83.5% of the children failed the test according to our criteria and only 16.5% passed [Figure 1]. The passing criteria of TEOAE were: (a) The response was reproducible 50% of times the test was performed; and (b) Any of the three frequencies tested (1.0, 1.5, 2.0, 3.0, 4.0 kHz) had 3 dB more power in the response spectrum than the noise spectrum.
DISCUSSION
There are several issues in the assessment of hearing in children with CP and these include the objective test to be chosen as per needs of the child, reliability of these tests, degree of hearing loss, and its precise localization.
In our study, prevalence of hearing loss in children with CP was calculated from patients on the basis of children who failed on BERA. The prevalence was found to be 41.5%. However, the actual prevalence would still be higher because this does not take into consideration the cortical-level hearing loss. The exact prevalence of hearing loss can probably come only from CERA.
Topolska et al. in 2002 had performed audiologic examination on 32 patients. Their audiological testing comprised of impedance audiometry, DPOAE, BERA, and psychophysical studies—tonal and speech audiometry. They recognized hypoacusis in 37.5% of the children on the basis of psychophysical studies.11 They could not perform tonal audiometry in 25% of the cases due to the mental status of the child. Hearing impairment affects a significant proportion of children with CP.
Weir et al. (2018) performed audiologic assessment of 940 patients and found hearing loss in 367 (39%).12 They collected data from their AudGen Database, including pediatric patients with a diagnosis of CP. They collected data from the free field audiometry and ear-specific audiometry tests. According to this study, hearing loss of 15 dB or more on PTA or 20 dB by sound field audiometry was taken as significant. No BERA or OAE was done.
In most cases, there is evidence of involvement of cochlea, as OAE is absent in most cases (83.5%). Children who are BERA pass and OAE pass (14%) should hear normally. If they have hearing loss, it is because of a more central cause. Children who are BERA pass and OAE fail (44.5%) could have fluid in the middle ear or mild SNHL. Children who are BERA fail and OAE pass could have lesion at the spiral ganglion or brainstem or cochlear nerve. Children who are BERA fail and OAE fail (39%) could have purely cochlear or cochlear and brainstem/nerve involvement [Figure 2].
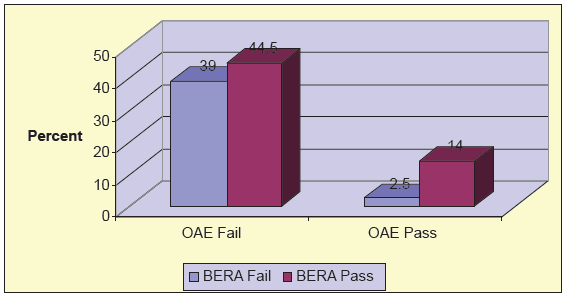
- Pattern of results of all ears tested. BERA: Brainstem evoked response audiometry, OAE: Otoacoustic emissions.
Taking BERA as gold standard, the efficacy of OAE was compared with it using the chi-square test. Chi-square value was 11.30 and p-value was 0. 0007. The difference between the two tests was statistically very significant. Hence, OAE was found to be a less efficacious test as compared to BERA in detecting hearing loss.
In the last few years, cochlear implants (CIs) have been developed for auditory rehabilitation of children having severe to profound hearing loss.13 Richard et al. (2021) did a systematic review and identified two interventions (hearing aid and cochlear implantation).14
Rehabilitation in the form of hearing aid or CI would be required in children who are OAE fail and BERA fail (39%), OAE fail and BERA pass (44.5%), and OAE pass and BERA fail (2.5%).
The children in our study group hardly ever got hearing aids fitted because parents were already occupied with multiple other handicaps of the child. Rehabilitation of hearing loss still remains an unachievable goal in such children with CP.
There are various issues in the assessment of hearing of children with CP. They are unable to speak and respond, so it becomes difficult to ascertain whether hearing loss actually exists. If the hearing loss is due to a defect in hearing pathway before the cortex, the child is expected to improve with hearing aids, CIs, or brainstem implants. However, if this is at cortical level, none of the above-mentioned devices would work. Hence, it is important to establish, quantify, and find the level of defect, and this is a difficult task.
Correlation of results of TEOAE/DPOAE, BERA, PTA with hearing in cerebral palsy
Our results were categorized in six groups:
-
1.
Hearing present—TEOAE/DPOAE present—BERA pass—PTA OK/not possible
No intervention for hearing is required in this group of children. They require speech training only.
-
2.
Hearing present—TEOAE/DPOAE absent—BERA fail—PTA OK/not possible
There is no explanation for this scenario. Maybe the tests are unreliable. Nevertheless, no intervention is required for hearing. They require speech training.
-
3.
Hearing deranged—TEOAE/DPOAE absent—BERA threshold raised/fail—PTA threshold raised/not possible
Such children will benefit from hearing aids/CI and speech training. We also need to treat any conductive element if present.
-
4.
Hearing absent—TEOAE/DPOAE present—BERA fail—PTA no response/not possible
Such children could be helped with CI/brainstem implants.
-
5.
Hearing absent—TEOAE/DPOAE present—BERA pass—PTA no response/not possible
CERA could give answers for this group of children. No intervention can be done.
-
6.
Hearing absent—TEOAE/DPOAE absent—BERA fail—PTA no response/not possible
CI/brainstem implant could help.
Issues in implanting children with cerebral palsy having hearing loss
These children suffer multiple handicaps. The result of speech even after treating hearing handicap remains unpredictable. The high cost of CI puts a burden on the already financially strained family. None of these children in our group were implanted.
Newer modalities like growth hormone administration have found some success in the recovery of hearing but needs exploration.15
CONCLUSION
The prevalence of hearing loss amongst CP children was calculated to be 41.5%. In most cases, the site of lesion was found to be cochlea, as OAE was absent in most of such cases (83.5%). OAE was found to be a less efficacious test as compared to BERA in detecting hearing loss.
Authors’ contributions
NNM, EN: Contributed in the concept, design, the definition of intellectual content, literature search, clinical study, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review. Both authors take responsibility for the integrity of the work as a whole from inception to published article.
Ethical approval
The research/study complies with the Helsinki Declaration of 1964.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing of the manuscript and no images were manipulated using AI.
REFERENCES
- A report: The definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007;109:8-14.
- [PubMed] [Google Scholar]
- Prevalence, type, distribution, and severity of cerebral palsy in relation to gestational age: A meta-analytic review. Dev Med Child Neurol. 2008;50:334-40.
- [CrossRef] [PubMed] [Google Scholar]
- An update on the prevalence of cerebral palsy: A systematic review and meta-analysis. Dev Med Child Neurol. 2013;55:509-19.
- [CrossRef] [PubMed] [Google Scholar]
- Encephalopathies. In: Behrman RE, Kliegman RM, Jennson HB, eds. Nelson textbook of pediatrics. Philadelphia: Saunders; 2005. p. :2024-25.
- [Google Scholar]
- A population-based study and systematic review of hearing loss in children with cerebral palsy. Dev Med Child Neurol. 2011;53:1038-45.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of severe hearing impairment in a population-based cerebral palsy cohort. Pediatr Neurol. 2014;51:641-4.
- [CrossRef] [PubMed] [Google Scholar]
- Hipoacusia neurosensorial en pacientes con parálisis cerebral [Sensorineural hearing loss in cerebral palsy patients] Acta Otorrinolaringol Esp.. 2006;57:300-2.
- [CrossRef] [PubMed] [Google Scholar]
- The frequency of other handicaps in children with cerebral palsy. Dev Med Child Neurol. 1973;15:305-12.
- [CrossRef] [PubMed] [Google Scholar]
- Sensorineural hearing loss in patients with cerebral palsy after asphyxia and hyperbilirubinemia. Int J Pediatr Otorhinolaryngol. 2005;69:1211-7.
- [CrossRef] [PubMed] [Google Scholar]
- Developmental – behavioral pediatrics. In: Basil JZ, Holly WD, eds. Atlas of pediatric physical diagnosis. Philadelphia: Mosby; 1997. p. :58-86.
- [Google Scholar]
- Ocena słuchu u dzieci z mózgowym porazeniem dzieciecym. Porównanie badań subiektywnych i obiektywnych [Assessment of hearing in children with infantile cerebral palsy. Comparison of psychophysical and electrophysical examination] Otolaryngol Pol. 2002;56:467-74.
- [PubMed] [Google Scholar]
- Hearing Loss in Pediatric Patients With Cerebral Palsy. Otol Neurotol. 2018;39:59-64.
- [CrossRef] [PubMed] [Google Scholar]
- Hearing rehabilitation in cerebral palsy: Development of language and hearing after cochlear implantation. Braz J Otorhinolaryngol. 2015;81:240-7.
- [CrossRef] [PubMed] [Google Scholar]
- Hearing Loss Diagnosis and Early Hearing-Related Interventions in Infants With or at High Risk for Cerebral Palsy: A Systematic Review. J Child Neurol. 2021;36:919-29.
- [CrossRef] [PubMed] [Google Scholar]
- Early treatment with growth hormone (GH) and rehabilitation recovers hearing in a child with cerebral palsy. Reports. 2019;2:4.
- [CrossRef] [Google Scholar]



