
Translate this page into:
Attention Deficit Hyperactivity Disorder and dopamine D4 receptor (DRD4) polymorphisms in South Indian population
* Corresponding author: Chillal Guru Prasad, Department of Psychiatry, Bangalore Medical College and Research Institute, Bangalore, India. Email: imgurunimhans@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Chillal GP, Shivappa M, Jain S, Girimaji S, Purushottam M. Attention Deficit Hyperactivity Disorder and dopamine D4 receptor (DRD4) polymorphisms in South Indian population. Ann Natl Acad Med Sci (India). 2024;60:157–63. doi: 10.25259/ANAMS-2022-1-16-(452)
Abstract
Objectives
Four decades of research have found that Dopamine D4 Receptor (DRD4) is the major candidate gene however, few studies have supported the association between the DRD4 exon III long seven repeat allele and Attention Deficit Hyperactive Disorder (ADHD). Two Indian studies had shown there is an association between DRD4 7 repeat allele; hence, we investigated in the south Indian population. AIMS: To study the association of DRD4-EXON-3-7R long allele and minor physical anomalies with ADHD in comparison to age & sex-controlled normal subjects with no evidence of ADHD. settings and design-cross-sectional case-control study for two years at National Institute of Mental Health And NeuroSciences, Bangalore.
Material and Methods
60 children with ADHD and 60 healthy children of 4-16 years of age group were recruited after informed consent. Assessed by DSMIV-TR, ADHD RS IV HOME VERSION 18 items, comorbidities by detailed interview of child and parents using Mini-International Neuropsychiatric Interview for Children & Adolescents (M.I.N.I). Kid for minor congenital anomalies modified waldrop scale & for the perinatal complications, Lewis Murray Obstetrics Complication Scales were applied. For the family history family interview for genetic study, global functioning was measured by children global assessment scale, neuropsychological tests of response inhibition test were used and blood samples was collected for genotyping.
Results
The genotype 2 2,2 4 ,4 4,4 5,4 7 repeat allele has shown equal distribution between cases and controls with p-value 0.492 with no significance.
Conclusion
There is no association between DRD4 EXON-3-7R long allele gene polymorphism and ADHD in South Indian population. DRD4 7R could be having influence on minor physical anomalies in ADHD.
Keywords
ADHD-Attention Deficit Hyperactivity Disorder
DRD4 7R – Dopamine D4 Receptor 7Repeat allele
VNTR – Variable Number Tandem Repeats

Introduction
Attention deficit hyperactivity disorder (ADHD) is a neuropsychiatric problem with onset in early childhood.ADHD is a condition characterized by inattention, impulsivity or both, and hyperactivity with onset before the age of seven years, giving rise to significant academic, social, and emotional problems at home and at school.1
ADHD is a polygenic disorder with more than 30 dopaminergic, noradrenergic, serotonergic, and gamma-aminobutyric acid neurotransmitter genes known to contribute to its susceptibility. Evidence of genetic susceptibility comes from several studies on a repertoire of genes, including Dopamine D4 Receptor (DRD4), dopamine receptor, DRD5, dopamine beta-hydroxylase gene, Serotonin transporter Gene (5HTT), 5HydroxyTryptamine Receptor 1B Gene (HTR1B), and Synaptosomal Associated Protein of 25kDa (SNAP25).2 In India, there is very little systematic research on ADHD in children.3
Meta-analysis has shown a statistically significant association between ADHD and dopamine system genes, especially DRD4 and DRD5.4 Four decades of research have found that DRD4 is the major candidate gene, however, few studies failed to support the association between the DRD4 exon III long seven repeat allele and ADHD.3,4,5
Dopamine is the key neurotransmitter in the development of ADHD. Evidence to support dopaminergic dysfunction in ADHD derives from three research areas: the neuropharmacology of stimulant medication4,6 the behavior and biochemistry of animal models, and neuroimaging studies in ADHD adults.4 Various meta-analyses have shown consistent evidence of the association of many candidate genes with childhood ADHD. Significant associations were identified for several candidate genes including DAT1, DRD4, DRD5, 5HTT, HTR1B, SNAP25, and also significant heterogeneity was observed for DBH, ADRA2A, 5HTT, TPH2, and MAO-A.4,6,7,8 From 1991 to 2004, including three genome-wide linkage studies and association studies of 94 polymorphisms in 33 candidate genes.Evidence for association exists for four genes in ADHD: the dopamine D4 and D5 receptors and the dopamine and serotonin transporters.9 Family association studies examined genetic components in the etiology of ADHD by using the Transmission Equilibrium test for the association between ADHD and DRD4 7R allele.4
As heritability is high, there is a 2–8-fold increase in risk for ADHD in children whose parents had ADHD, while twin studies attribute 80% of the etiology to genetic factors. The mean heritability estimates of 76% amongst twins indicate ADHD is the most heritable psychiatric disorder.4
Minor physical anomalies (MPAs) are congenital abnormalities of body structure as they develop from the same ectoderm layer in the embryo, which reflect fetal maldevelopment. MPAs are markers of central nervous system anomalies. High MPA counts have been associated with hyperactive behavior in normal boys and with inhibited behavior in normal girls.10
DRD4 STRUCTURE AND FUNCTION
The dopamine D4 receptor structurally and pharmacologically resembles the dopamine D2 and D3 receptors. The dopamine D4 receptor gene is located on chromosome 11p15.511,12 and contains a remarkable number of polymorphic regions. There is a hypervariable region in the third cytoplasmic loop of the dopamine D4 receptor gene consisting of 2–10 imperfect 48 base pair repeats.13 Therefore, the D4 receptor isoforms differ in the length of the third cytoplasmic loop and have 1, 4, 7, or 11 times the same insert of a stretch of 16 amino acid residues in their protein structure. The dopamine D4.2, D4.4, and D4.7 receptor alleles occur the most frequently, the ancient polymorphisms14 but there is considerable variation in the distribution of alleles depending on ethnicity.14,15 The universality of the polymorphism with only three common repeat-number alleles (4, 7, and 2) indicates that the polymorphism is ancient and arose before the global dispersion of modern humans. Various meta-analysis studies have shown varying genetic associations of DRD4 with ADHD.
INDIAN CONTRIBUTION
An Indian study has found that ADHD transmission of different polymorphisms of the DRD4 in different ethnic groups. Bhaduri et al. study in 2006 is the first report on the transmission of different polymorphisms of DRD4 in Indian subjects.The transmissions of 6 and 7 repeat alleles of exon 3 48-bp Variable Number Tandem Repeats (VNTR) showed a significant association with ADHD.16 Das M et al. study in 2011 showed significant preferential transmission of the 7R-T (DRD4 exon3 VNTR-rs1800955) and 3R-T (MAOA-u VNTR-rs6323).17 Haplotypes were noticed from parents to probands of East Indian population. However, Stanley et al. (2017)’s Mumbai-based study has failed to support the association between the DRD4 exon III long seven repeat allele.18 There is a paucity of Indian studies to generalize the association between DRD4 and ADHD in Indian population, hence this study was conducted.
MATERIAL AND METHODS
After getting approval from the Institutional Ethics Committee of National Institute of Mental Health and Neurosciences Bangalore, assent from children with written informed consent from parents was taken.
Study design: Cross-sectional case–control study.
Inclusion criteria: Cases of 60 children aged 4–16 years who were diagnosed to have ADHD as per DSM-IV TR from inpatient & outpatient of child and adolescent psychiatry services. sixty controls of children aged 4–16 years with no ADHD were recruited from Indira Gandhi Institute of Child Hospital, Bangalore.
Exclusion criteria: Children with identifiable dysmorphic syndrome, pervasive developmental disorders, any form of mental retardation including Fragile-X syndrome, and any serious systemic illness like cardiac, renal, or liver failure were excluded.
Phenotype assessment
Mini Kid developed by David Sheehan et al. was used for brief structured diagnostic interviews for children and adolescents within 15 min. Children under 13 years of age were interviewed in the presence of their parents.19
Modified Waldrop Minor Congenital Anomaly Scale: This scale assesses MPAs of the head, eyes, ears, mouth, hands, and feet, as it takes only 15 min with very minimal removal of clothing. It’s a simple instrument with good inter-rater reliability and inter-scorer agreement. The coefficient of correlation of the scale has been found to be +0.84.20
Lewis Murray Obstetrics Complication Scale (LMOCS) rates 15 obstetric complications as absent or definitely present; 9 items of the exposure can also be rated as equivocally present. It provides a measure of perinatal insults that may affect brain development from case notes, birth records, and maternal interviews.21
Family Interview for Genetic Study (FIGS) is a guide for gathering genetic diagnostic information about relatives in the pedigrees being studied.22
-
ADHD-Rating Scale IV Home Version (ADHD-RSIV) is a revised version that can be completed by either parents (home form) or teachers (school form). There are two subscales, Inattentive and Hyperactive/Impulsive subscale. It can be administered to 4–20 years old. The test has good psychometric properties, particularly reliability and discriminant validity, making it especially useful for clinical samples. The ADHD RS-IV has high utility for multiple applications due to its quick completion, easy scoring, and sensitivity to treatment that was used to measure Inattentivity and Hyperactivity/Impulsivity in children.23,24
Response Inhibition Test.
Stroop Color Word Interference Test: These measures selective attention, cognitive flexibility, and processing speed. In this test, subjects have to read the names of colors, naming colors, and naming color names that are printed in the color chart. The score is the amount of time needed by the subject to correctly identify the items per page and the number of errors committed. The last task has an interference component because it requires the subject to override or inhibit a reading response. It is a measure of executive functioning, cognitive flexibility, and the ease with which a person can shift his or her perceptual set to conform to changing demands and inhibit usual response from interfering with the unusual one.25 An increase in Stroop interference is seen in ADHD.
Go/No – Go TEST is a measure of one’s ability to suppress reflexes motor impulses and is done in two parts. First, the subject has to get into the set with contrasting movements, i.e., when the examiner shows one finger, the subject has to show two, and when the examiner shows two fingers, the subject has to show one. The sequence of movements is performed with the dominant hand. The subject is instructed that the rules would be changed, i.e., when the examiner shows two fingers, the subject has to show one finger, and when the examiner shows one finger, the subject has to do nothing. The correct responses, as well as the errors, are noted and form the score, which was used to measure a child’s ability to suppress reflexes and motor impulses.26
Children’s Global Assessment Scale Score (CGAS) (Schaffer et al. 1983)27 an instrument that provides a global measure of level of functioning in children and adolescents. It is designed to reflect the lowest level of functioning for a child or adolescent during a specific time period. The measure provides a single global rating, on a scale of 0–100, where scores above 70 indicate normal function. In rating, the clinician makes use of the glossary details to determine the meaning of the points on the scale. This assesses current functioning and retrospective measures of the highest past functioning and the worst past functioning for a period of 1 month. The reliability has been reported to be kappa = 0.61 (Hanssen-Bauer et al. 2007).28
METHODOLOGY
Genotyping
Five (5) ml of venous blood drawn from subjects under aseptic conditions & DNA was isolated from leukocytes nuclei by salting out method (Miller et al. 1988).29
Principle
Detergents can solubilize lipids in the cell and nuclear membranes, thus releasing DNA into solution. High salt helps in the precipitation of the excess protein in the solution. The residual protein is further degraded by the addition of a special kind of protease called Proteinase K. High-molecular weight DNA is precipitated using cold absolute ethanol.
DRD4 gene is extremely polymorphic. It has one polymorphism located in the third exon coding for the third cytoplasmic loop of the receptor and consisting of a variable number of copies ofa 48 base pair sequence, from 2 to 10.
Primers flanking the third cytoplasmic loop repeat region were used for Polymerase Chain Reaction (PCR).
Forward primer -- 5′TGTGGTGTAGGGAACGGCCTGAG 3′
Reverse primer -- 5′CTTCCTGGAGGTCACGGCTCAAGG3′30
Polymerase chain reaction (PCR) was carried out for 30 cycles along with thermostable DNA polymerase enzyme, TAQ POLYMERASE, at an annealing temperature of 61°C, and then products were resolved on 2.5% agarose gel, fragment sizes were determined by comparison with molecular weight, standards, and tested for 2, 4, 5, and 7 repeat alleles of DRD4 exon 3–48 base pairs.
Statistical Analysis
The data sheets were coded and analyzed using descriptive statistics such as means, frequency distributions, percentages, and standard deviation. For continuous variables, the parametric Student’s ‘t’ test was used to compare the means between the two groups andnon-parametric. There is an increase in MPAs and DRD4 present ADHD cases.
Tests such as chi-square, and Mann–Whitney U test were used for categorical variables through Statistical Package for Social Sciences (SPSS13.0).
Hardy–Wienberg equilibrium states that the genetic variation in a population will remain constant from one generation to the next in the absence of disturbing factors (p2+ q2+ 2pq = 1). It was checked in all sample distribution of genotypic & allelic frequencies and were compared in cases and controls using chi-square test. The group was in Hardy -Weinberg equilibrium. The data does not follow the Test of Normality (Kolmogorov -Smirnov Z), so the non-parametric tests were used.
RESULTS
Male 49 (81) Female 11 (19) ADHD RS-IV: Attention Deficit Hyperactive Disorder Rating Scale IV; CGA score: Children’s Global Assessment Scale Score; SD: Standard deviation. Cases Mean & SD Controls Mean & SD * p value is significant at 0.05; SD: Standard Deviation. SD: Standard Deviation. * p value significant <0.05. DRD4: Dopamine Receptor D4. * p value significant < 0.05; LMOC: Lewis Murray Obstetrics Complication. ADHD RS-IV: Attention Deficit Hyperactive Disorder Rating Scale IV; DRD4 7R – Dopamine D4 Receptor 7Repeat allele. MPA: Minor physical anomalies; DRD4 7R – Dopamine D4 Receptor 7Repeat allele.
Mean (in months) & SD
Results (%)
Age of onset ADHD
31.05 (13.73)
Age of 1st assessment
70.87 (32.71)
ADHD RS-IV severity
34.95 (10.23)
p = 0.0001
CGA score
59.83 (11.57)
Scales
Results
Waldrop minor congenital anomaly scale
3.67 (1.90)
2.0 (1.27)
p = 0.0001*
Lewis-Murray obstetric complication scale
0.45 (1.26)
0.02 (0.13)
p = 0.010*
Cases Mean (s) & SD
Controls Mean (s) & SD
Results
139.75 (39.15)
106.64 (24.19)
0.009*
Genotype alleles
Cases
Controls
Frequency
Percentage (%)
Frequency
Percentage (%)
2 2
0
0
3
5
2 4
6
10
4
6.7
4 4
49
81.7
48
80
4 5
1
1.7
1
1.7
4 7
4
6.7
4
6.7
Pearson chi-square test
p-value = 0.492. No significance.
Case
Controls
Mann– Whitney U
p-value significance
Waldrop score
75.48
45.52
907
0.0001*
LMOC score
67.54
53.46
1377
0.0001*
DRD4 7 repeat
ADHD RS-IV score
Mean ranks
Mann–Whitney u
Significance
Present
4
38.75
79
0.349
Absent
56
29.91
DRD4 7 repeat
Waldrop score
Mean ranks
Mann–Whittney U
Significance
Present
4
29.63
63.5
0.143
Absent
56
42.62
DISCUSSION
There is a gap between the onset and first consultations of 32 months, which is consistent with Malhi et al.’s study, as shown in Table 1.3 ADHD subtypes—combined were 76.6%, 18.3% of inattentive, 1.7% of hyperactive-impulsive, and 3.3% of residual type, among which males were higher in numbers which is consistent with Malhi et al.’s study.3 It showed higher rates of ADHD in males as compared to females, which varies between 3 and 7:1, in our study, the M:F is 4:1 which is consistent with the Mukhopadhyay et al. study.31 The ADHD RS IV score in DRD4 7R cases present was 38.75, whereas it was 29.91 in the DRD4 7R absent cases. Though this was not statistically significant, but there appears to be a trend of greater severity of ADHD in the presence of DRD 4 7R allele.
The Child Global Assessment Score (CGAS) in cases had shown a Mean of 59.83 in variable functioning with sporadic difficulties or symptoms in several but not in all areas. Disturbance would be apparent to those who encounter the child in a dysfunctional setting or time but not to those who see the child in other settings.
The majority of studies on ADHD have supported a strong familial nature of this disorder as 2–8-fold increase in the risk for ADHD in parents and siblings of children with ADHD. In fact, the mean heritability was shown to be 76% (Bovincini et al., 2020),4 which is comparable to other neuropsychiatric disorders such as schizophrenia or bipolar disorder. Butin our study, we had 11.6% of cases with a family history of any psychiatric illnesses, among which 3.3% had ADHD, which is the least, as we have not done the familial genetic analysis.
In ADHD, it is shown that there are higher rates of MPAs and obstetrical complications, which have been reported in those with inattention and hyperactive behaviors. In our study, Waldrop minor congenital anomaly score (p = 0.0001) and Lewis Murray Obstetric Complication score (p = 0.01) showed significant differences between cases and controls in Table 2 and consistent with Fogel CA et al.’s study.10
An increase in stroop interference shown by meta-analysis which was tested by using stroop color word interference test. In the neuropsychological test, 81.7% of cases completed the Stroop test, and 19.3% (those who could not do the Stroop test) were administered the go-no-go test. In the control group, 90.0% could complete the Stroop test, and the remaining 10% did the go-no-go test. There was a statistically significant difference between the cases and controls [Table 3]. 28.8% had specific learning disorders, 26.6% had expressive language disorder, and seizure disorders were 21%. This is consistent with the studies by Bush, Lansbergen, and Lopez et al.32-34
In our study [Table 4, Figure 1], the VNTR alleles of the DRD4 gene exon 3 found include 2-repeat (R), 4R, 5R, and 7R alleles. We have found 4R allele is the highest which is 81% and is consistent with the worldwide prevalence of 64.3% (Polanczyk G et al. 2007).1 The second highest is longer 7R with about 6.7% but the global prevalence is 20.6% and it differs in Americans with 48.3%, and least in Southeast Asia with 1.9%. The third most common is the shorter 2R allele which is 5% in our study, as compared to global prevalence of 8.2%, and it has shown to be highest in Southeast Asia (18.1%). None of the alleles were significantly associated with ADHD cases, which is consistent with one Mumbai-based study (Stanley et al. 2017) and 42 similar studies shown in the meta-analysis of Bonvicini, Gizer et al.’s study.4,35-37 However, 34 studies and 2 Indian studies (Bhaduri, Das M et al.) on subjects from Eastern India has shown an association of DRD4 Exon3-7R and ADHD (Bonvicini, Wang, Gizer, Sánchez-Soto, Li et al.).4,16,17,35-40 These results indicate a possible difference in the allele frequencies of the DRD4 VNTR’s across different ethnic groups.
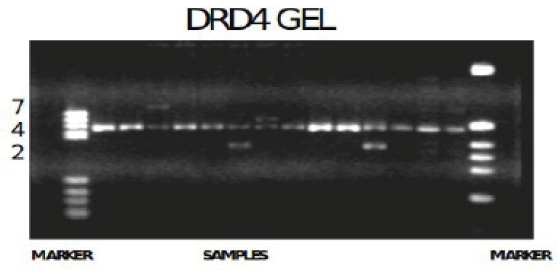
- Variable Number Tandem Repeats (VNTR) polymorphism fragments of DRD4 7repeat allele gene photograph.
- Lanes 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
- This is the photograph of the 2.5% agarose gel showing the DRD4 7R gene alleles under ultraviolet illumination, after the completion of gel electrophoresis. The sizes were determined after comparing the allele size with standard marker which was loaded in the agarose gel, along with the amplified polymerase chain reaction (PCR) products of the subjects. In the above photograph, the marker is present on the left- and right-hand side. Lanes 1,16- Bands were compared with standard DNA marker 1-PBR, 16- Haelll Digest
- Lanes 2,3,5,6,9,10,11,13,14,15- genotype of 4 4
- Lane 4 ----------------------------- genotype of 4 7
- Lanes 7, 12 ----------------------------- genotype of 2 4
- Lane 8 ----------------------------- genotype of 2 2
In Table 5, the mean Waldrop score (p = 0.0001*) and mean Lewis Murray Obstetrics Complication Scale (LMOCS) score (p = 0.0001*) was higher in the cases as compared to controls, which is statistically significant. Table 6 shows mean ranks between the DRD4 7R present and absent group in cases with ADHD RS-IV score. On Mann–Whitney U non-parametric test, there is no significant difference, which is consistent with Fogel CA et al.10 There was no association between DRD4 7 repeat allele and ADHD. In Table 7, there is no significant association between MPA and DRD4 7R allele. The MPAs are indicating that some early embryonic either genetic or non-genetic had played a role in the genesis of ADHD in this population.
STRENGTHS
The researchers were blind to the genotyping of the sample, and the accuracy was 99.52%. There was no ethnicity problem, as all subjects in the study were South Indians. The current study adds to the knowledge of the present status of DRD4 7R allele and the ADHD, given the fact that ADHD is a polygenic disorder with variable environmental influence.
LIMITATIONS
In view of the low sample size, the influence of predictor variables, like psychosocial adversities, could not be analyzed. Chances of type II error are high due to the small sample size. Hence, the generalizability of the finding to our population is difficult and needs further validation with a larger diverse sample size and family-based studies to find any significant association of the DRD4 7 R allele with ADHD.
CONCLUSION
Cases with DRD4 7R allele had a non-significantly higher mean rank of ADHD RS-IV score but no association.
In our study, there is no association between DRD4 7R and ADHD.
Acknowledgments
Thanks to all the participants and Indira Gandhi Institute of Children Hospital, Bangalore
Ethical approval
The research/study approved by the Institutional Ethics Committee of National Institute of Mental Health and Neurosciences Bangalore, number NIMHANS 59th 59 IEC/8.09/21-05-2008.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am J Psychiatry. 2007;164:942-8.
- [CrossRef] [PubMed] [Google Scholar]
- Genetics of attention deficit hyperactivity disorder. Mol Psychiatry. 2019;24:562-75.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Spectrum of Attention deficit hyperactivity disorders in children among referrals to Psychology services. Indian Paediatr. 2000;37:1256-60.
- [PubMed] [Google Scholar]
- DRD4 48 bp multiallelic variants as age-population-specific biomarkers in attention-deficit/hyperactivity disorder. Transl Psychiatry. 2020;10:70-89.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- ADHD and the DRD4 exon III 7-repeat polymorphism: An international meta-analysis. Soc Cogn Affect Neurosci. 2010;5:188‐93.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Different effects of the DRD4 genotype on intrinsic brain network connectivity strength in drug-naïve children with ADHD and healthy controls. Brain Imaging Behav. 2022;16:464-75.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Candidate gene studies of ADHD: A meta-analytic review. Hum Genet. 2009;126:51‐90.
- [CrossRef] [PubMed] [Google Scholar]
- A meta-analysis of association studies between the 10-repeat allele of a VNTR polymorphism in the 3’-UTR of dopamine transporter gene and attention deficit hyperactivity disorder. Am J Med Genet B Neuropsychiatr Genet. 2007;144B:541‐50.
- [CrossRef] [PubMed] [Google Scholar]
- Molecular genetic studies of ADHD: 1991 to 2004. Am J Med Genet B Neuropsychiatr Genet. 2005;132B:109‐25.
- [PubMed] [Google Scholar]
- Hyperactive behavior and minor physical anomalies. Acta Psychiatr Scand. 1985;72:551-6.
- [CrossRef] [PubMed] [Google Scholar]
- The D4 dopamine receptor (DRD4) maps to distal 11p close to HRAS. Genomics. 1992;13:208‐10.
- [CrossRef] [PubMed] [Google Scholar]
- The D4 dopamine receptor gene maps on 11p proximal to HRAS. Genomics. 1993;18:161‐3.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple dopamine D4 receptor variants in the human population. Nature. 1992;358:149‐52.
- [CrossRef] [PubMed] [Google Scholar]
- An historical perspective on “The world-wide distribution of allele frequencies at the human dopamine D4 receptor locus”. Hum Genet. 2014;133:431-3.
- [CrossRef] [PubMed] [Google Scholar]
- A hypervariable segment in the human dopamine receptor D4 (DRD4) gene. Hum Mol Genet. 1993;2:767‐73.
- [CrossRef] [PubMed] [Google Scholar]
- Association of dopamine D4 receptor (DRD4) polymorphisms with attention deficit hyperactivity disorder in Indian population. Am J Med Genet B Neuropsychiatr Genet. 2006;141B:61‐6.
- [CrossRef] [PubMed] [Google Scholar]
- Role of gene-gene/gene-environment interaction in the etiology of eastern Indian ADHD probands. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35:577‐87.
- [CrossRef] [PubMed] [Google Scholar]
- DRD4 and DAT1 VNTR genotyping in children with attention deficit hyperactivity dsorder. Indian J Clin Biochem. 2017;32:239‐42.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) J Clin Psychiatry. 2010;71:313-26.
- [CrossRef] [PubMed] [Google Scholar]
- Hyperactivity and minor physical anomalies in elementary school children. Am J Orthopsychiatry. 1971;41:602-7.
- [CrossRef] [PubMed] [Google Scholar]
- Obstetric complications, neurodevelopmental deviance, and risk of schizophrenia. J Psychiatr Res. 1987;21:413-21.
- [CrossRef] [PubMed] [Google Scholar]
- Family interview for genetic studies. FIGS manual, Illinois (IL): Northwestern Health Care; 1992:August 3.
- ADHD Rating Scale-IV: Checklists, norms, and clinical interpretation. New York (NY): Guilford Press; 1998.
- Parent and teacher ratings of attention-deficit/hyperactivity disorder symptoms: Factor structure and normative data. Psychol Assess. 2016;28:214-25.
- [CrossRef] [PubMed] [Google Scholar]
- Higher cortical functions in man. New York (NY): Basic Books; 1966.
- A children’s global assessment scale (CGAS) Arch Gen Psychiatry. 1983;40:1228-31.
- [CrossRef] [PubMed] [Google Scholar]
- Inter-rater reliability of clinician-rated outcome measures in child and adolescent mental health services. Adm Policy Ment Health. 2007;34:504-12.
- [CrossRef] [PubMed] [Google Scholar]
- A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988;16:1215.
- [CrossRef] [PubMed] [Google Scholar]
- Protocadherins: A large family of cadherin-related molecules in central nervous system. EMBO J. 1993;12:2249-56.
- [CrossRef] [PubMed] [Google Scholar]
- Attention deficit hyperactivity disorder. Indian J Pediatr. 2003;70:789-92.
- [CrossRef] [PubMed] [Google Scholar]
- Attention-deficit/hyperactivity disorder and attention networks. Neuropsychopharmacol. 2010;35:278-300.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Stroop interference and attention-deficit/hyperactivity disorder: A review and meta-analysis. Neuropsychology. 2007;21:251-62.
- [CrossRef] [PubMed] [Google Scholar]
- Usefulness of the Stroop test in attention deficit hyperactivity disorder. Rev Neurol. 2010;50:333-40.
- [PubMed] [Google Scholar]
- The genetic architecture of selection at the human dopamine receptor D4 (DRD4) gene locus. Am J Hum Genet. 2004;74:931-44.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Relations between multi-informant assessments of ADHD symptoms, DAT1, and DRD4. J Abnorm Psychol. 2008;117:869-80.
- [CrossRef] [PubMed] [Google Scholar]
- Revisiting the functional role of dopamine D4 receptor gene polymorphisms: Heteromerization-dependent gain of function of the D 4.7 receptor variant. Mol Neurobiol. 2019;56:4778-85.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Common and specific genes and peripheral biomarkers in children and adults with attention-deficit/hyperactivity disorder. World J Biol Psychiatry. 2018;19:80-100.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Attention-deficit hyperactivity disorder in adults: A systematic review and meta-analysis of genetic, pharmacogenetic and biochemical studies. Mol Psychiatry. 2016;21:872-84.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Meta-analysis shows significant association between dopamine system genes and attention deficit hyperactivity disorder (ADHD) Hum Mol Genet. 2006;15:2276-84.
- [CrossRef] [PubMed] [Google Scholar]



