
Translate this page into:
Cathelicidin Antimicrobial Peptide (CAMP) and Its Correlation with Serum 25 Hydroxy Vitamin D in Under-Five Children with Pneumonia
Address for correspondence Piyush Gupta, MD, FIAP, Department of Pediatrics, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, New Delhi 110095, India (e-mail: prof.piyush.gupta@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Cathelicidins are human peptides involved in innate immunity, and are believed to be mediators of vitamin D-related immune benefits. We aimed to evaluate the correlation between serum levels of 25 hydroxy vitamin D (25(OH)D) and serum cathelicidin antimicrobial peptide (CAMP) in children hospitalized with severe pneumonia. This was a secondary analysis from a larger randomized double-blind placebo-controlled trial on vitamin D supplementation in severe pneumonia. Children aged 6 months to 5 years with the World Health Organization (WHO) defined severe pneumonia were included. Any child with rickets, immunodeficiency, or chronic illness was excluded. Baseline serum CAMP, serum 25(OH)D, and immunoglobulins were measured and analyzed. A total of 163 under-five children were recruited with mean (standard deviation) age 16.4 (13.0) months. The median (interquartile range [IQR]) serum CAMP was 12.5(8.0–20.0) ng/mL and serum 25(OH)D was 14.4 (8.4–24.2) ng/mL. There was no significant correlation between serum cathelicidin and serum 25(OH)D (r = −0.064, p = 0.415). Serum 25(OH)D was low (<20 ng/mL) in 105(64.4%) participants. Median (IQR) serum CAMP was comparable between children with low (<20 ng/mL) and normal serum 25(OH)D levels (13.0 [8.2, 22.1] and 12.0 [8.0, 17.4] pg/mL; p = 0.2). Serum cathelicidin showed significant positive correlation with serum immunoglobulin M levels (r= 0.456, p < 0.001). There was no significant correlation between serum cathelicidin and serum vitamin D in under-five children hospitalized with severe pneumonia.
Keywords
cathelicidin
vitamin D
infection
children
pediatric

Introduction
Cathelicidin antimicrobial peptides (CAMP) are a group of antimicrobial peptides that are released on leukocyte activation and cause disintegration of cell membranes of microorganisms. They act through multiple receptors including toll-like receptors and chemokine receptor type 4 on neutrophils to chiefly affect apoptosis, phagocytosis, cellular migration, and cytokine release.1 Cathelicidins maintain equilibrium during an inflammatory response by its proinflammatory and anti-inflammatory properties and potential for angiogenesis and epithelial wound repair. They contribute to innate immunity and defense against inhaled organisms in the lungs.2 Poor CAMP response is reported in various diseases like tuberculosis, sarcoidosis,3 and asthma.4 Few adult studies have documented defensive role of CAMP in bacterial infections of respiratory tract caused by intracellular microorganisms.5
The transcription of cathelicidin gene is postulated to be affected by active form of vitamin D (1,25 dihydroxy vitamin D). Therefore, low CAMP levels have been reported in vitamin D deficiency states.6 Vitamin D supplementation has shown to increase cathelicidin levels in experimental studies.7,8 However, data from these studies is limited by lack of clinical data for inference, small sample size, and differences in populations that were assessed. The validity of this correlation, if any, has not been tested in clinical setting of infections in populations that are vitamin D-deficient per se.
We, thus, undertook this study to evaluate the levels of serum CAMP in under-five children with pneumonia from Northern India as per their vitamin D status. We also wanted to ascertain if there existed any correlation between CAMP and serum 25 hydroxy vitamin D (25(OH)D) in children with active infection.
Methods
These data were collected as part of a randomized double-blind placebo-controlled trial that evaluated efficacy of single oral mega-dose of vitamin D3 for treatment and prevention of pneumonia in hospitalized under-five children.9 The original trial was approved by Institutional Ethical Committee (including collection of blood for the parameters analyzed in this study; Trial Registration: CTRI/2013/01/003317). Children aged 6 months to 5 years with a clinical diagnosis of severe pneumonia (defined as presence of lower chest indrawing in children presenting with cough or difficult breathing) were assessed for enrolment after hospitalization.10 Children with rickets, chronic illness including immunodeficiency, and those with a recent consumption history of vitamin D or calcium supplements were excluded.
A baseline serum sample was collected for estimation of serum calcium, phosphate, alkaline phosphatase (ALP), serum 25(OH)D, intact parathyroid hormone (iPTH), and immunological markers (serum immunoglobulin IgA, IgG, IgM, and CAMP. Blood samples for 25(OH)D and PTH were collected and transported in ice immediately to an in-house testing laboratory. Serum PTH and serum 25(OH)D were estimated by radioimmunoassay using commercially available kit manufactured by Immunotech SAS, Marseille, France (interassay variation: below or equal to 10·3%; intra-assay variation: below or equal to 7·7%; sensitivity: 2 pg/mL) and DiaSorin, United States (interassay variation: 11%; intraassay variation: 12·5%; sensitivity: at or below 1·5 ng/mL), respectively. Vitamin D sufficiency, insufficiency, and deficiency (VDD) were diagnosed at serum 25(OH)D more than 20 ng/mL, 12 to less than or equal to 20 ng/mL and less than 12 ng/mL, respectively.11 Systematic sampling method was followed to measure immunological markers in every alternate child in view of available logistic support. Serum CAMP was estimated using a standard commercial kit (Human LL-37, HK 321 Hycult Biotech, the Netherlands [sensitivity: 0·1 ng/mL], based on sandwich enzyme immunoassay (enzyme-linked immunosorbent assay [ELISA]). Serum immunoglobulins (IgA, IgG, and IgM) were measured quantitatively with immunoenzymatic colorimetric method using ELISA-based kits (Xema Co Ltd, Russia) having a sensitivity of 0·12 g/L.
All children were managed as per standard protocol10 and were monitored 8 hourly during hospitalization. The child was discharged when fever and fast breathing were absent for at least 24 hours. The duration of hospitalization (hours) and time to resolution of pneumonia (hours) defined as abatement of fever and fast breathing were recorded.
Statistical Analysis
Data were analyzed using SPSS version 20.0. Quantitative variables like biochemical and immunological markers were depicted as median and interquartile range (IQR). The strength of correlation between serum CAMP and 25(OH)D and immunological markers (nonparametric data) was measured using Spearman correlation (r). Statistical significance was at p-value less than 0.05
Results
Total 324 children were recruited in the original trial. Baseline data on immunological markers was available for 163 children with mean (standard deviation [SD]) age of 16.4 (13.0) months. The median (IQR) cathelicidin levels were 12.5(8.0–20.0) ng/mL. The median (IQR) levels of serum 25(OH)D, iPTH, and ALP were 14.43 (8.42–24.17) ng/mL, 25.71 (13.85–58.54) pg/mL, and 208 (158–291.5)IU/L, respectively. The median (IQR) levels of serum immunoglobulins IgA, IgG, and IgM were 0.84 (0.59–1.21), 7.36 (5.39–9.66), and 2.59 (1.65–4.11) mg/dL, respectively. The proportion of vitamin D sufficiency, insufficiency, and VDD were 58 (35.6%), 39 (23.9%), and 66 (40.5%), respectively.
Serum CAMP showed an inverse but insignificant correlation with serum 25(OH)D (r= −0.064, p = 0.415; ►Fig. 1) and iPTH (r= −0.03, p = 0.710). Among immunoglobulins, serum CAMP showed significant positive correlation with serum IgM (r = 0.456, p < 0.001, ►Fig. 2) unlike IgA (r= −0.05, p = 0.49) and IgG (r= 0.05, p = 0.54). Serum CAMP levels were not related to age (r = 0.03), severity of pneumonia (r = 0.13), duration of hospitalization (r = 0.05), and time to resolution of pneumonia (r = 0.10; p > 0.05). Weight for height had an inverse correlation with serum CAMP (r = −0.09; p = 0.67).
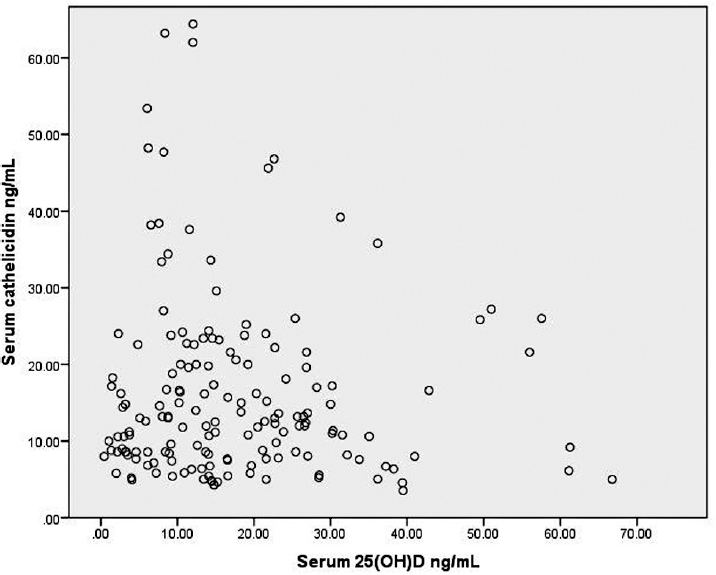
- Correlation between serum cathelicidin and serum 25-hydroxy vitamin D (25 (OH)D) levels (n = 162).
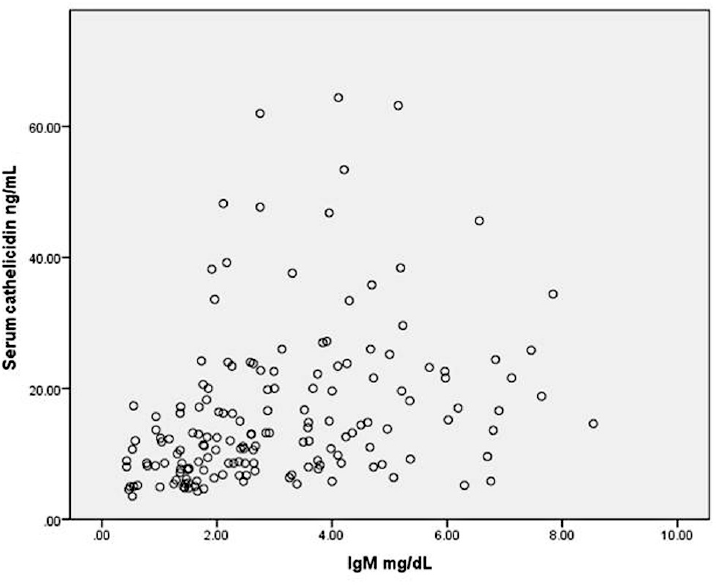
- Correlation between serum cathelicidin and serum immunoglobulin M (IgM) levels (n = 162).
►Table 1 compares the laboratory parameters between those with and without vitamin D sufficiency. There was no significant correlation between serum CAMP and serum 25(OH)D in either of the groups (r= −0.235, p = 0.08 and r= 0.028, p = 0.77), respectively. Serum CAMP correlated significantly with serum IgM (r = 0.36, p < 0.001) in those with vitamin D insufficiency (≤20 ng/mL). Serum CAMP correlated significantly with both IgM and IgG (r = 0.6, p < 0.001 and r = 0.27, p = 0.040), respectively, in those with vitamin D sufficiency.
| Parameter | Serum 25(OH)D <20ng/mL (n = 105) | Serum 25(OH)D ≥20ng/mL (n = 58) | p-Value |
|---|---|---|---|
| Age, mo | 12 (7, 25) | 11 (7.8, 18) | 0.752 |
| Serum cathelicidin, ng/mL | 13.0 (8.2, 22.1) | 12.0 (8.0, 17.4) | 0.447 |
| Serum 25 (OH) D, ng/mL | 10.2 (6, 14.2) | 27.6 (23.1, 37.5) | <0.001 |
| Serum parathyroid hormone, pg/mL | 34.2 (14.3, 74.6) | 19.7 (13.3, 31.8) | 0.002 |
| Serum calcium, a mg/dL | 8.6 (8.0, 9.1) | 8.7 (8.2, 9.2) | 0.878 |
| Serum phosphorus, a mg/dL | 5.0 (4.0, 5.7) | 4.5 (4.0, 5.6) | 0.062 |
| Serum Alkaline phosphatase, IU/L | 237 (164, 335) | 184.5 (148.8, 213.8) | 0.005 |
| Serum IgA, mg/dL | 0.86 (0.55, 1.23) | 0.81 (0.62, 1.0) | 0.752 |
| Serum IgG, mg/dL | 7.0 (5.2, 9.0) | 7.5 (6.7, 10.2) | 0.583 |
| Serum IgM, mg/dL | 2.6 (1.8, 4.1) | 2.6 (1.4, 4.6) | 0.916 |
Abbreviations: 25 (OH D, 25 hydroxy vitamin D; IgA, immunoglobulin A; IgG, immunoglobulin G; IgM, immunoglobulin M; IQR, interquartile range.
Data represented as median (IQR).
a n = 60 and 30 in first and second group, respectively.
Discussion
In this study, under-five children hospitalized with pneumonia were evaluated and found to have an insignificant inverse correlation between serum cathelicidins with serum 25(OH)D. Low serum vitamin D levels were present in majority of these children.
Cathelicidins exhibit a dual role in systemic inflammation by acting as proinflammatory or anti-inflammatory molecules.12 Its levels may be beneficial in infections like pneumonia, meningitis, and skin infection but detrimental in severe sepsis.12 A significant positive correlation was seen between cathelicidin and serum IgM levels reiterating the proinflammatory role in acute pneumonia. This correlation remained significant irrespective of the vitamin D levels.
Data on quantitative level of serum cathelicidin and its association with 25(OH)D in infection has been contentious. Low cathelicidin levels were reported earlier among healthy adults with low (<32ng/mL) serum 25(OH)D levels.13,14 Lower serum cathelicidins with low vitamin D levels were associated with poorer lung function among adults with pneumonia.15 Conversely, higher cathelicidin values with low serum 25(OH)D levels were reported among 30 neonates with congenital pneumonia.16 Vitamin D modulates the immune response by its effect on CD4+ T cells and attenuation of proinflammatory response.17 The higher median levels of cathelicidins in those with lower 25(OH)D levels and negative correlation between the two were seen in this study. This is similar to a recent study in hospitalized adults with coronavirus disease 2019 pneumonia, where CAMP LL-37 levels were higher in those with pneumonia than healthy controls. The cathelicidin levels further decreased after vitamin D supplementation at day 7 and day 14.18 This suggests the proinflammatory role of cathelicidins in infection and a declining trend with vitamin D supplementation. The vitamin D levels were reported as lower in critically sick children19 that can independently affect the clinical outcomes in an adverse manner. An understanding of the association with other antimicrobial peptides can help to decipher the role of vitamin D supplementation in sick children.
The results of our study should be interpreted considering insufficient vitamin D levels in most children. Second, the cohort comprised of children with acute respiratory infection. Inclusion of a comparative healthy control group could have improved understanding of these biochemical associations. This study was not statistically powered to conclude a significant association between cathelicidin and serum vitamin D levels as it was a secondary analysis of collected data.
To conclude, serum cathelicidins showed poor correlation with serum 25(OH)D levels in hospitalized children with acute pneumonia, but correlated with immunoglobulin levels suggesting their role in inflammation. Future studies are required to ascertain the role of vitamin D in systemic inflammatory response in childhood pneumonia.
Any Previous Presentation of the Manuscript
We declare that manuscript has not been previously published nor is not being considered for publication elsewhere.
Authors' Contribution
PG, DS, PD, and AKB contributed to study design and conceptualization. AD and NK were involved in data acquisition and analysis. Initial draft was written by AD and NK. The manuscript was revised with critical inputs from DS, PD, AKB, and PG. All authors have read and approve the final content of the manuscript.
Conflict of Interest
Zuventus Healthcare Ltd. India was involved in procurement of vitamin D administered in the original trial. This manuscript does not bear any conflict of interest with the firm. The pharmaceutical company did not influence data acquisition, analysis, or drafting of the manuscript.
Funding
Grant awarded to Principal Investigator Dr Piyush Gupta by Indian Council of Medical Research.
References
- Cathelicidin impact on inflammatory cells. Cent Eur J Immunol. 2015;40(02):225-235.
- [CrossRef] [PubMed] [Google Scholar]
- The human cathelicidin LL-37: a multifunctional peptide involved in infection and inflammation in the lung. Pulm Pharmacol Ther. 2005;18(05):321-327.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D, cathelicidin, prolactin, autoantibodies, and cytokines in different forms of pulmonary tuberculosis versus sarcoidosis. Isr Med Assoc J. 2017;19(08):499-505.
- [Google Scholar]
- The association of vitamin D, cathelicidin, and vitamin D binding protein with acute asthma attacks in children. Allergy Asthma Proc. 2015;36(04):51-58.
- [CrossRef] [PubMed] [Google Scholar]
- Serum concentrations of antimicrobial peptide cathelicidin LL-37 in patients with bacterial lung infections. Cent Eur J Immunol. 2018;43(04):453-457.
- [CrossRef] [PubMed] [Google Scholar]
- Calcitriol stimulates gene expression of cathelicidin antimicrobial peptide in breast cancer cells with different phenotype. J Biomed Sci. 2016;23(01):78.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanisms of action of vitamin D as supplemental therapy for pneumocystis pneumonia. Antimicrob Agents Chemother. 2017;61(10):e01226-e17.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of cholecalciferol supplementation on vitamin D status and cathelicidin levels in sepsis: a randomized, placebo-controlled trial. Crit Care Med. 2015;43(09):1928-1937.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D supplementation for treatment and prevention of pneumonia in under-five children: a randomized double-blind placebo controlled trial. Indian Pediatr. 2016;53(11):967-976.
- [CrossRef] [PubMed] [Google Scholar]
- Pocket Book of Hospital care for children: guidelines for the management of common illnesses with limited resources. 2005 at: http://www.who.int/maternal_child_adolescent/documents/9241546700/en/ (accessed )
- [Google Scholar]
- Indian Academy of Pediatrics Revised (2021) guidelines on prevention and treatment of vitamin D deficiency and rickets. Indian Pediatr. 2022;59(02):142-158.
- [CrossRef] [PubMed] [Google Scholar]
- The dual role of cathelicidins in systemic inflammation. Immunol Lett. 2017;182:57-60.
- [CrossRef] [PubMed] [Google Scholar]
- Positive correlation between circulating cathelicidin antimicrobial peptide (hCAP18/LL-37) and 25-hydroxyvitamin D levels in healthy adults. BMC Res Notes. 2012;5:575.
- [CrossRef] [PubMed] [Google Scholar]
- Circulating levels of 25-hydroxyvitamin D and human cathelicidin in healthy adults. J Allergy Clin Immunol. 2011;127(05):1302-4.e1.
- [CrossRef] [PubMed] [Google Scholar]
- A cross sectional analysis of the role of the antimicrobial peptide cathelicidin in lung function impairment within the ALIVE cohort. PLoS One. 2014;9(04):e95099.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic value of anti-microbial peptide, cathelicidin in congenital pneumonia. J Matern Fetal Neonatal Med. 2015;28(18):2197-2200.
- [CrossRef] [PubMed] [Google Scholar]
- Immunological aspects of SARS-CoV-2 infection and the putative beneficial role of vitamin-D. Int J Mol Sci. 2021;22(10):5251.
- [CrossRef] [PubMed] [Google Scholar]
- Rapid and effective vitamin D supplementation may present better clinical outcomes in COVID-19 (SARS-CoV-2) patients by altering serum INOS1, IL1B, IFNg, cathelicidin-LL37, and ICAM1. Nutrients. 2021;13(11):4047.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D deficiency in critically ill children: a systematic review and meta-analysis. Crit Care. 2017;21(01):287.
- [CrossRef] [PubMed] [Google Scholar]



