
Translate this page into:
Percutaneous Snaring and Retrieval of Cephalad Migrated Double J Stents in Pediatric Patients–A Bailout Technique Urologists Should Know

Address for correspondence Udit Chauhan, MD, PDCC, MNAMS, EBIR, Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Rishikesh 249203, Uttarakhand, India (e-mail: Dr.udit.chauhan@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Double J (DJ) stents are placed in patients with obstructive uropathy to relieve the obstruction. Curved ends prevent slippage or migration of the stent. Antegrade migration into the urinary bladder or retrograde migration into the ureter are common complications. Mode of retrieval of migrated stents depends upon the location of the stent. We present a case series of four cases with percutaneous snaring of cephalad migrated DJ stents in pediatric patients.
Keywords
migrated DJ stents
obstructive uropathy
snaring

Introduction
Double J (DJ) stents are commonly deployed in cases with post-pyeloplasty internal urinary diversion. Cystoscopy is a commonly used method of DJ stent removal. Caudal migration of the stent into urinary bladder is amenable to endoscopic retrieval. However, proximally migrated stents in the renal pelvis cannot be retrieved using cystoscopy or ureteroscopy. Ureteroscope-guided retrieval is further difficult in postoperative cases and in pediatric population due to difficult anatomy.1,2
We report four cases of percutaneous snaring of stents migrated cephalad into the renal pelvis.
Materials and Technique
Retrospective analysis of the cases was done after approval from Institute Medical Records Section. Cases with cephalad migrated ureteric DJ stents were searched in archive of old cases. Keywords used were “migrated ureteric stent” and “snare retrieval.” Four cases were selected which underwent stent retrieval with percutaneous snaring technique. All the cases were post-pyeloplasty patients of pelviureteric junction obstruction. Patients were referred for stent retrieval within first week of placement after failed ureteroscopic retrieval. Procedures were performed after an informed consent, under sedation as all the patients were young children. Time for administration and recovery from sedation were included in the procedure time. Fluoroscopic time and radiation dose were recorded in each case. All procedures were done using single plane frontal arm of Philips Allura HD (Philips, Amsterdam, the Netherlands). Procedural steps included ultrasound-guided calyceal puncture of affected kidney with 18G Chiba needle (Blueneem, Indiana, United States). 8F angiographic sheath (Arrow, Teleflex, North Carolina, United States) was placed to establish access. 5F Kumpe multipurpose catheter (Cook Medical, Indiana, United States) and J-tip 0.035” hydrophilic guidewire (Terumo, New Jersey, United States) were navigated into pelvicalyceal system. 5 mm diameter Amplatz Goose-Neck snare (Medtronic, Minnesota, United States) was used to capture and retrieve migrated stents. Snare was advanced over the snare sheath. The most important and challenging step of the procedure was stent engagement by snare (►Fig. 1A–E). Engagement was confirmed in fluoroscopy by movement of the stent upon snare manipulation. Coiled stents overlap with the snare. So, oblique views were employed to ensure adequate engagement and capture. Tightly looped stents were difficult to deal with. Fluoroscopic time increased in such cases.
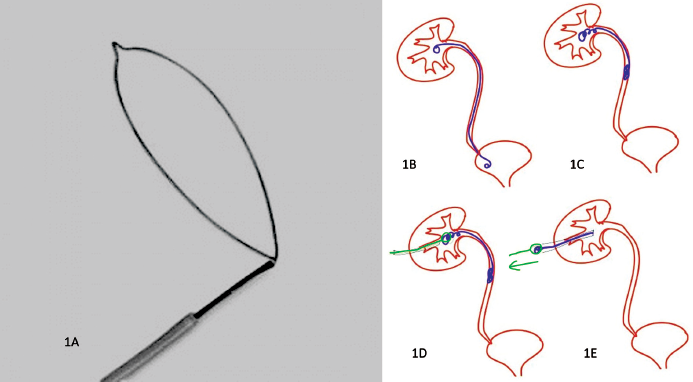
- Photograph of a snare (A). Schematic line diagrams showing a normal stent (drawn in blue) position (B) and a migrated double J stent (C), introduction of a snare with sheath (drawn in black and green) (D), engagement of the stent (D), and retrieval by the snare (E).
Stents were pulled out along with the catheter once engaged. Post-retrieval nephrostogram was obtained in all the cases to ascertain contrast leakage or any signs of injury. Patients were observed for post-procedural hematuria and other complications.
All stents were retrieved in first or second attempt. Dilated renal pelvis was favorable for maneuvering of snare and capturing the stent. Minimal dilated collecting system poses technical difficulty as space for maneuvering of the stent is less. Manipulation in such cases would damage the urothelium.
Case 1
A 3-year-old child was operated with Anderson-Hynes pyeloplasty for right-sided pelviureteric junction obstruction. A DJ stent was placed to relieve the obstruction. Post-procedure radiograph showed complete proximal migration and coiling of the stent in the renal pelvis. Ureteroscopic retrieval was attempted, and was unsuccessful as no part of the stent was accessible in urinary bladder or in the ureter. Patient was planned for percutaneous snaring of migrated stent. Stent was retrieved with a 5 mm (►Fig. 2A–D). No immediate or late post-procedure complications were observed. Total procedure time was 20 minutes and fluoroscopic time was 60 seconds. Dose area product was 505 mGy cm2.
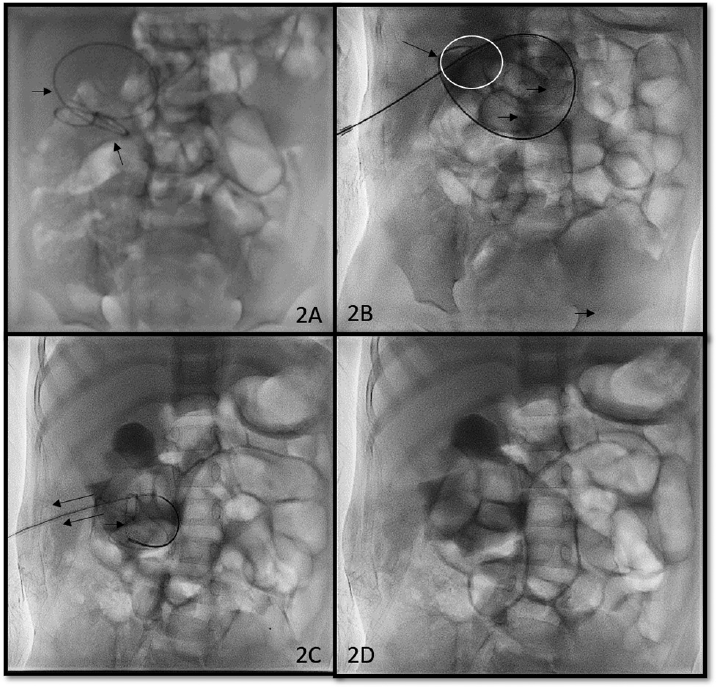
- Fluoroscopic spot image (A) of the upper abdomen region shows coiled migrated double J stent (short arrows) in the right renal area. Loop of snare (arrows) engages the stent (circle) in the lower pole region (B). Stent is being pulled with snare (arrows) (C). Post-procedure nephrostogram spot image (D) shows completely removed stent and no leakage of contrast from pelvicalyceal system.
Case 2
A 12-year-old boy with pelviureteric junction obstruction on right side underwent Anderson-Hynes pyeloplasty for pelviureteric obstruction. While placing the DJ stent, whole length of the stent migrated and coiled in the renal pelvis. Ureteroscope-guided retrieval was attempted, but was unsuccessful. So, to keep the diversion patent, another DJ stent was placed to avoid obstruction. Patient was planned for percutaneous snaring and retrieval of the migrated DJ stent. This case was technically challenging as the retrieval of the migrated stent was to be performed without displacing the second functioning stent (►Fig. 3A–D). Oblique fluoroscopic projections were used to deal with overlapping of two stents and capturing the migrated stent. Snare was maneuvered to separate the migrated stent. Migrated stent was caught by the snare and was later pulled out. No immediate or late post-procedure complications were seen. The second stent remained functioning. Total procedure time was 25 minutes and fluoroscopic time was 50 seconds. Dose area product was 490 mGy cm2.

- Fluoroscopic spot image (A) of the KUB region shows coiled up migrated double J (DJ) stent in right renal area (asterisk) along with normally positioned another DJ stent (short arrows). Nephrostogram images (B and C) show loop of snare engaging migrated DJ stent (circle) and stent is being pulled out (long arrows) through sheath without displacing normally placed DJ stent (short arrows). Post-procedure spot image (D) shows intact normally placed DJ stent. No leakage of contrast seen from pelvicalyceal system after snaring.
Case 3
An 8-year-old boy with left-sided pelviureteric junction obstruction underwent Anderson-Hynes pyeloplasty for pelviureteric obstruction. During placement, upper end of the stent migrated into the renal pelvis and lower end migrated into the distal ureter. Patient was planned for percutaneous snaring and retrieval of the migrated DJ stent. Stent was engaged by the snare and was later pulled out along with (►Fig. 4A–C). No immediate or late post-procedure complications were seen. Dilated renal pelvis allowed maneuvering of the snare and engagement of the stent without much technical difficulty. Total procedure time was 30 minutes and fluoroscopic time was 80 seconds. Dose area product was 750 mGy cm2.

- Nephrostogram image (A) of the KUB region shows coiled up migrated double J (DJ) stent in left renal area (short arrows). Renal pelvis is dilated. Upper end of stent is caudally migrated. Images (B and C) show loop of snare engaging migrated DJ stent (circle) and the migrated DJ stent being pulled with snare (long arrows) through sheath.
Case 4
A 10-year-old girl with right-sided pelviureteric junction obstruction underwent Anderson-Hynes pyeloplasty for pelviureteric obstruction. During the procedure, upper end of the stent migrated into the renal pelvis and lower end into the distal ureter. Stent formed a tight loop within the renal pelvis. Dilatation of the pelvis was minimal. This allowed less manipulation with the snare. Stent was engaged by the snare and was later pulled out along with. No immediate or late post-procedure complications were seen. Total procedure time was 35 minutes and fluoroscopic time was 120 seconds. Dose area product was 980 mGy cm2.
Discussion
Since first use in 1967, DJ stents are commonly used in to decompress the obstructed pelvicalyceal system. Post-pyeloplasty DJ stent placement is done to avoid obstruction at anastomotic site secondary to postoperative edema, clots, or fibrotic stricture formation. Migration of the stents is common in caudal direction into the urinary bladder.1 Cephalad migration into renal pelvis or collecting system is uncommon. Reported incidence of cephalad migration is 0.6 to 3.5%.2
Common technique for the removal of cephalad migrated stents is ureteroscopy-guided retrieval. Other methods used are ureteric balloon dilators, percutaneous forceps, and basket.2,3 Shin et al performed percutaneous antegrade removal or exchange of DJ stents with the help of a snare or a basket catheter. They treated 27 patients (39 stents) with a technical success rate of 95%.4 They used 9-Fr sheath to access the collecting system and used 6 mm angioplasty balloon for retrieval and manipulation. Use of larger sheath and balloon may injure the urothelium. In our case series, angioplasty balloon was not used. Manipulation with snare did not result in post-procedure hematuria. Percutaneous retrieval was done with 8F sheath and 5F catheter, which are more compliant and less traumatic than forceps or balloon dilators.
Liang et al treated 24 patients (26 stents) with 100% technical success rate5 using forceps or snare. All patients without a pre-existing percutaneous nephrostomy (8 patients) had undergone retrieval of their DJ stents by forceps. In this case series, without a pre-existing nephrostomy tube, retrieval of the migrated stent by snare was successful.
Yeung et al treated 20 patients with fluoroscopically-guided stent retrieval with a success rate of 85%.6 Out of the 17 procedures, two procedures (12%) were performed with a snare.
Conclusion
Percutaneous snaring is a safe and effective technique in appropriate setting and favorable anatomy. It can retrieve stents migrated into renal pelvis, which are inaccessible with ureteroscopy. Use of oblique fluoroscopic projections facilitates effective capture by the snare. Limited and careful maneuvering and manipulation of the snare avoid urothelial injury and subsequent complications.
Details of Earlier Presentation
None.
Authors' Contributions
Khanak Nandolia was involved in data collection, data analysis and interpretation, and drafting of the article. Udit Chauhan contributed to conception or design of the work, data analysis and interpretation, and critical revision of the article.
Conflict of Interest
None.
Funding
None.
References
- A rare case of double J stent migration in the kidney. Urol Case Rep. 2021;36:101557.
- [CrossRef] [PubMed] [Google Scholar]
- Retrieval of proximally migrated ureteral stents. J Urol. 1992;148(04):1205-1206.
- [CrossRef] [PubMed] [Google Scholar]
- Ureteroscopic retrieval of proximally located ureteral stents. Urology. 1991;37(05):446-448.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous antegrade removal of double J ureteral stents via a 9-F nephrostomy route. J Vasc Interv Radiol. 2007;18(09):1156-1161.
- [CrossRef] [PubMed] [Google Scholar]
- Antegrade retrieval of ureteral stents through an 8-French percutaneous nephrostomy route. AJR Am J Roentgenol. 2008;191(05):1530-1535.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous fluoroscopically guided removal of dysfunctioning ureteral stents. Radiology. 1994;190(01):145-148.
- [CrossRef] [PubMed] [Google Scholar]



